This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
[link] A 30 year-old woman was brought to the ED with chestpain. It had started just after nursing her newborn, about an hour prior, and she described it as a severe non-pleuritic “pressure” radiating to the back. She had given birth a week ago, and she had similar chestpain during her labor. Lobo et al.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. Pericarditis?
The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiac arrest. Anterolateral STEMI. The formula results in 23.43, just above the 23.4 He was defibrillated. Here is his post resuscitation ECG: Now the diagnosis is obvious.
After dinner the day of presentation, she had left neck and elbow pain which she described as dull, achy, and worse with exertion. She contacted her neighbor, a nurse, for help. See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. The patient presented to triage at around 10 PM. At midnight.
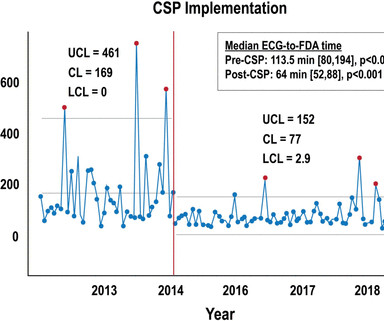
A comprehensive iSTEMI protocol (CSP) was implemented on 15 July 2014, incorporating: (1) cardiology fellow activation of the catheterisation lab using standardised criteria, (2) nursingchestpain protocol, (3) improved electronic access to electrocardiographic studies, (4) checklist for initial triage and management, (5) 24/7/365 catheterisation (..)
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. He had been awakened by cough at 3 AM 2 days earlier.
A late middle-aged man presented with one hour of chestpain. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 It would be difficult to get a nurse to give it faster!
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
The patient was a 70-something yo previously healthy male on no medications who presented to the ED with epigastric pain, onset over a few hours. He denied chestpain of any sort and his vitals were all normal. The STEMI criteria in normal conduction are only 75% sensitive for OMI!!
One of my most talented readers is a health care assistant (a nursing assistant) who has taken a keen interest in ECGs. Now chestpain free. Trop T now very high, well into the range one sees with a STEMI; very unusual in type II MI. And they teach me a lot. He can beat nearly anyone. You don't have to be a genius.
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. A 59 y/o Female calls 911 for crushing chest discomfort and difficulty breathing.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the Emergency Department with sudden onset chestpain that began 14-hours ago. The nurse alerted the MD because the patient was still symptomatic, diaphoretic and “looking unwell”.
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent").
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content