This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
A 50-something man presented in shock with severe chestpain. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Posterior wall involvement attenuates predictive value of ST-segment elevation in lead V4R for right ventricular involvement in inferior acute myocardialinfarction.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
There is no way to tell the difference between GI etiology of chestpain and MI. Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chestpain are nearly diagnostic of ischemia. An emergency cardiac ultrasound could be very useful.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. No pericardial effusion on ultrasound." PEARL: Most patients who present with new chestpain + ECG changes + positive troponin — will not need Cardiac MRI. What do you think?
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." Type 2 is more difficult to appreciate on angiography than type 1.
He was given aspirin and sublingual nitro and the pain resolved. Bedside cardiac ultrasound with no obvious wall motion abnormalities. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. This confirms that the pain was ischemia and is now resovled.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chestpain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. On medic arrival, she walked out of the house in no distress, but was diaphoretic.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. This was a point of care ultrasound, not a bubble contrast echo.
The term MINOCA stands for Myocardialinfarction with non-obstructive coronary arteries. A 50-year-old lady was admitted to my hospital with crushing chest tightness. Cardiac Causes Myocarditis – an infection of the heart may cause damage to the heart muscle and cause chestpain.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) The patient said his chestpain was 4/10, down from 8/10 on presentation. HsTnI drawn at that time was 9 ng/L (ref. 80%) and definitely too much for hour to hour.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 Annals of Emergency Medicine 2012;60:45-56. QRS V2 = 15.5
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. A emergent cardiology consult can be helpful for equivocal cases.
Both of these patterns together suggest Aslanger's pattern , recently published in J Electrocardiology: A new electrocardiographic pattern indicating inferior myocardialinfarction. Case Continued Bedside ultrasound was performed: This shows an anterior wall motion abnormality, and highly suggests the LAD as the infarct artery.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Smith comment: This patient did not have a bedside ultrasound. In fact, bedside ultrasound might even find severe aortic stenosis. What should be done?
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think? Gray, A., &
and European societal guidelines that intravascular imaging with either optical coherence tomography (OCT) or intravascular ultrasound (IVUS) should be routinely used during complex coronary stent procedures, s ays first authorGregg W. These results extend the strong recommendations from recent U.S.
A late middle-aged man presented with one hour of chestpain. Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. Most recent echo showed EF of 60%.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. If detected early by ultrasound, the patient can be saved. There was some SOB. He had walked into the ED (did not use EMS). 3) Oliva et al. (3)
No chestpain. His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. Later on during the night of his admission he had a short episode of chestpain that resolved with sublingual nitroglycerin.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. If detected early by ultrasound, the patient can be saved. There was some SOB. He had walked into the ED (did not use EMS). Obviously there is MI. Hammill SC.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. First, the name (MyocardialInfarction or Not) is not important.
History : An extremely elderly patient who lived independently presented with acute "oppressive" chestpain 7/10 in severity that was not positional, pleuritic, or reproducible. Appearance of Abnormal Q Waves Early in the Course of Acute MyocardialInfarction: Implications for Efficacy of Thrombolytic Therapy.”
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chestpain, dyspnea and weakness on the treadmill. In the ED he had some continued chestpain and hypotension. 5 of 6 presented with chestpain and an ECG indicating reperfusion therapy, but were detected by bedside ultrasound.
A man in his early 30s was walking when he developed central chestpain which was non-radiating, then had a syncopal event with bowel incontinence, and when he woke up he had ongoing chestpain. Notes never having symptoms like this before, pain is so severe its causing SOB. He called 911. So this is "MINOCA".
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. orthostatic vitals b.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. And almost all of them could be detected by bedside ultrasound. Not all chest discomfort is the same.
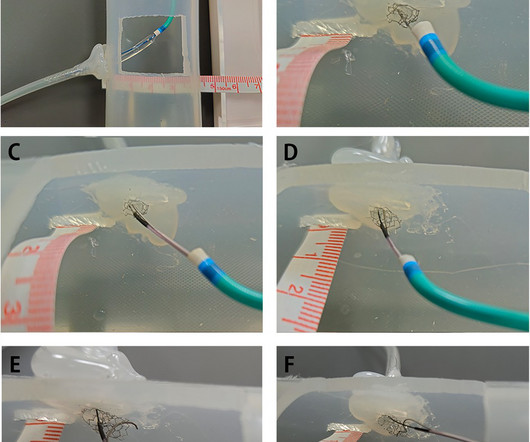
In this article, we introduce a dual-lumen microcatheterfacilitated wiring technique performed on two patients to overcome this difficulty.Case summaryThe first case was a 75-year-old man who presented with chestpain. The second case was a 78-year-old woman diagnosed with non-ST segment elevation myocardialinfarction.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Who seriously believes that the portion of myocardium that infarcted did not matter?
A middle-age woman with no previous cardiac history called 911 for chestpain. On arrival in the ED, a bedside ultrasound showed poor LV function (as predicted by the Queen of Hearts) with diffuse B-lines. This was her prehospital ECG: What do you think? I don't know what the device algorithm interpretation stated.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content