This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
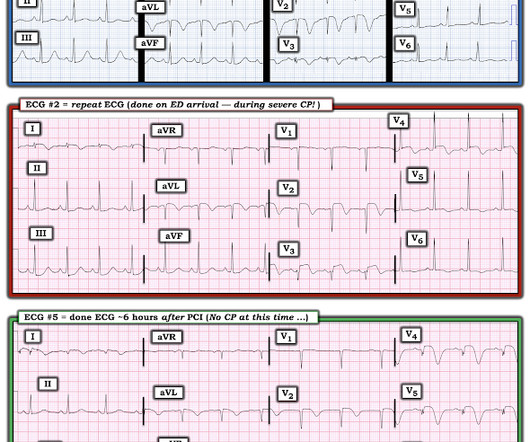
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The i nitial hs troponin I returned 75%.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered. Am J Emerg Med.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Jernberg T, et al.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Incidence of an acute coronary occlusion. Am J Med 2019, 132(5):622-630.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Below are two examples of this.
The ECLIPSE trial shows that use of IVI to guide coronary stenting in severely calcified lesions prevents death, stent thrombosis, and unplanned repeat procedures in this high-risk patient population. The ECLIPSE trial results were presented at the American College of Cardiology Scientific Session (ACC.25)
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. Patients on dialysis often do not have chestpain in the setting of acute MI. Why is this?
Case An elderly patient had acute chestpain and 911 was called. Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. What do you think? Khan AR, Golwala H, Tripathi A, et al.
BackgroundAcute myocardialinfarction commonly occurs in patients with coronary artery disease, but rarely, it can develop under a hypercoagulable state. Repeat coronary angiography confirmed recurrent thrombosis in the right coronary artery. These thrombotic complications predominantly arise in veins rather than in arteries.
IntroductionThe simultaneous occurrence of acute myocardialinfarction (AMI) and venous thromboembolism (VTE) is rare and often associated with underlying malignancies. Subsequent investigations revealed pulmonary embolism, deep vein thrombosis, and imaging findings suggestive of pancreatic cancer.
This was texted to me by a paramedic while I was out running one day: "54 yo male chestpain started at 1pm. Let's see how the PMCardio Queen of Hearts AI Model performs: "Acute Occlusive MyocardialInfarction" She gave this a score of 1.0 (100% History of diabetes type II and stent placement in 2018. What do you think?
He denied chestpain. This was most likely acute thrombosis of a coronary artery resulting in OMI: The ECG changes were attributed to hyperkalemia. It is correct that he did not have chestpain, but we must remember that fully 1/3 of full blown STEMI do not present with chestpain. The dye don't lie".except
Angiography was technically challenging as the patient was receiving CPR, but the cardiologist suspected acute stent thrombosis and initiated cangrelor, although no repeat angiography was able to be obtained. He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. SanzRuiz, R.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content