This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. Electrocardiographic Manifestations: Acute posterior wall myocardialinfarction. Posterior myocardialinfarction: the dark side of the moon. This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! J Emerg Med 2001; 20:391-401.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. See these casese (and I have many others): First ED ECG is Wellens' (pain free).
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Am Heart J (1989) 117 : pp 657-665. de Zwaan C.,
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. Usefulness of automated serial 12-lead ECG monitoring during the initial emergency department evaluation of patients with chestpain. Ann Emerg Med 1998;31(1):3-11. Wang T, Zhang M, Fu Y, et al. Marti D et al.
We present a complex case of NSTEMI with multi-vessel coronary artery disease treated with PCI via the Carlino technique.Case Description:A 60-year-old female with a history of hypertension, diabetes mellitus, and ischemic heart disease presented with severe chestpain that radiated to the neck and was associated with nausea and vomiting.
Case An elderly patient had acute chestpain and 911 was called. Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. What do you think? Khan AR, Golwala H, Tripathi A, et al.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. hours when she called 911. These do NOT indicate late, subacute MI.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Incidence of an acute coronary occlusion. link] Harhash AA et al.
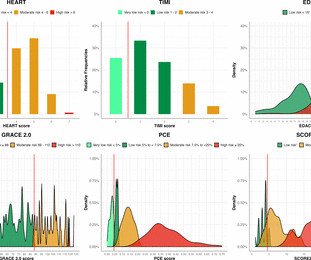
Background Guidelines recommend the use of risk scores to select patients for further investigation after myocardialinfarction has been ruled out but their utility to identify those with coronary artery disease is uncertain. The negative predictive value (NPV) varied from 77.3% –100%).
He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. This, in the context of worsening chestpain , is evidence of reocclusion of the infarct-related artery and active OMI in development. The below ECG was recorded.
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019.06.007) (Full text here: [link] ) The ECG above is diagnostic of Wellens' syndrome (full reference below): 1) Episode of anginal chestpain that is resolved (GONE!)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content