This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. Peak troponin was not recorded. Long term follow up is unavailable.
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). A woman in her late 70s presented with left arm pain. The arm pain started the day prior when she was at the dentist's office for a root canal. See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG.
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Former resident: "Just saw cath report, LAD stent was 100% acutely occluded."
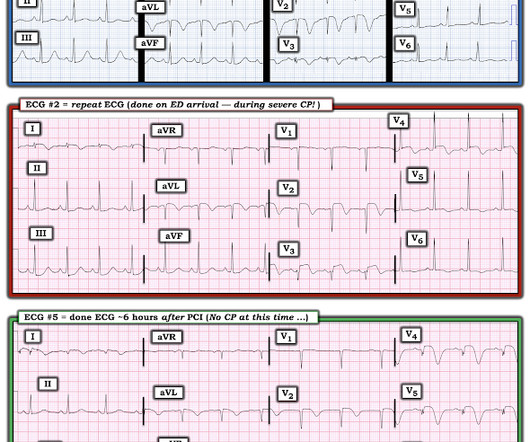
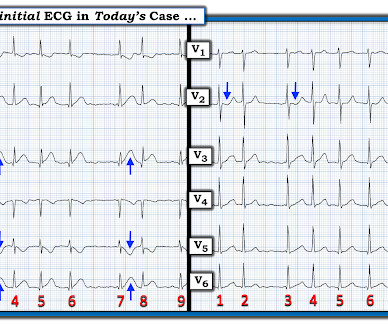
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). The ECG is diagnostic of occlusion myocardialinfarction (OMI). All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
A 50-something man presented in shock with severe chestpain. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Posterior wall involvement attenuates predictive value of ST-segment elevation in lead V4R for right ventricular involvement in inferior acute myocardialinfarction.
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. See this article by Widimsky: Primary angioplasty in acute myocardialinfarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy [link]
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
He underwent coronary stenting (uncertain which artery). There is no way to tell the difference between GI etiology of chestpain and MI. Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chestpain are nearly diagnostic of ischemia.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. A single DES stent was placed, and the patient did well post-procedure.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis?
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. Chestpain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Echo showed new anterior regional wall motion abnormality and decrease EF from 60% to 45%. Clin Cardiol 2022 4.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. He was treated for infection and DKA and admission to hospital was planned.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think? Gray, A., &
So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). The patient's chestpain had resolved by the time of the ECG 2. Angiogram: Widely patent RCA and LAD stents. The T-waves are flat.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. A stent was placed. Type B waves are deeper and symmetric. de Zwaan C.,
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
A 50 something male was seen in the emergency room due to typical chestpain. The pain had started the same day about two hours prior to medical contact. The medical care providers ascribed the patient's chestpain to new onset atrial fibrillation with rapid ventricular response after having viewed the ECG.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chestpain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. He had no h/o heart failure. DBT was 120 minutes, pretty good for a Non-STEMI OMI.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. You must record frequent serial ECGs for patients with chestpain.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) The patient said his chestpain was 4/10, down from 8/10 on presentation. RCA and PDA before and after, arrows indicating stented regions. Repeat ECG at that time is shown.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. link] Here is the history: A 30 yo man presented complaining of severe chestpain.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chestpain, nausea, vomiting and diffuse abdominal pain. It was stented. The patient was in DKA with an anion gap of 35, a glucose of 1128, and a K of 5.5
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
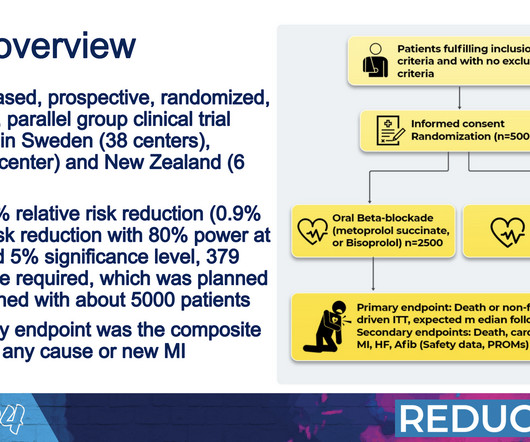
What we see today is more myocardialinfarctions that are smaller and that do not damage the heart muscle to the same extent.” Over a median follow-up period of 3.5 There were also no differences in safety endpoints such as stroke, abnormally low blood pressure or fainting.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content