This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
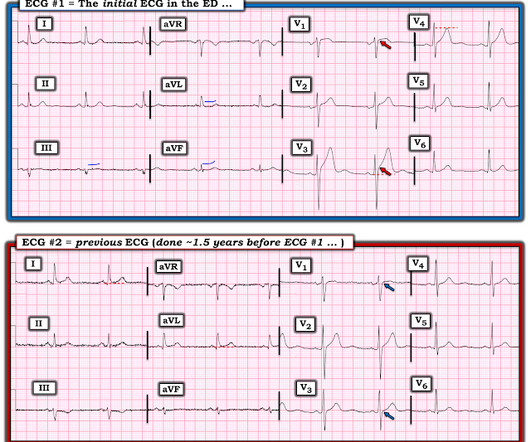
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. It was tested on a large database of known outcomes and was more than twice as senstivity as STEMI criteria and much better than cardiologists.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Written by Jesse McLaren A 65 year old with a history of atrial flutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chestpain, which was ongoing at triage. So a patient with high pretest probability (prior CABG with new chestpain), had new ECG changes showing posterior OMI.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). The ECG is diagnostic of occlusion myocardialinfarction (OMI). All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Smith : "What was the outcome?" x the QRS amplitude in any of V1-V4.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
A 29 year old male presented with 6 hours of stuttering chestpain, constant for the last hour, worse with breathing. Take home point here : Obtain an ECG on anyone with chestpain. 3) Q-waves are independently associated with worse outcomes (78% relative increase in 90-day mortality in Armstrong et al.)
A 50-something man presented in shock with severe chestpain. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. The patient was in clinical shock with a lactate of 8.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? hours earlier? Pol Arch Intern Med. 2017;127:401–411.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. Electrocardiographic Manifestations: Acute posterior wall myocardialinfarction. Posterior myocardialinfarction: the dark side of the moon. This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! J Emerg Med 2001; 20:391-401.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
BackgroundRecent evidence highlights an increasing incidence of myocardialinfarction in young women. years]) admitted to the China ChestPain Center Database between 2016 and 2021. years]) admitted to the China ChestPain Center Database between 2016 and 2021.
BackgroundHighsensitivity cardiac troponin (hscTnI) assays can quantify troponin concentrations with low limits of detection, potentially expediting and enhancing myocardialinfarction diagnoses. The primary outcome was hospital length of stay. Journal of the American Heart Association, Ahead of Print.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS.
This case was texted to me by one of our residency graduates, and with the outcome, so I don't know how I would have interpreted it blindly. A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. The highest ST/S ratio is in V3, and is 2.5/13
Risk ratios (RRs) and mean differences with 95% CIs were computed for binary and continuous outcomes, respectively.RESULTS:Five randomized controlled trials with a total of 5727 patients were included, of whom 51.1% 1.10];P=0.198), nonfatal myocardialinfarction (RR, 1.09 [95% CI, 0.63–1.88];P=0.768),
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
How frequent and whether outcomes are worse for patients with atypical presentation in acute coronary syndrome (ACS) across the literature is not known. We conducted a systematic review of the literature on patients with ACS or acute myocardialinfarction who reported whether their symptoms were atypical or typical.
A 67 yo f developed chestpain this morning." Opiates are associated with worse outcomes in MyocardialInfarction. See this case: A man his 50s with chestpain. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative.
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. He described the pain as a “crushing and discomforting” feeling with no radiation.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Wellen's syndrome is a Reperfusion syndrome.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chestpain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. Angiogram: "ACS - Non ST Elevation MyocardialInfarction. This is a HUGE myocardialinfarction.
There was a good outcome. We believe this represents a form of “toxicomythology” given the millions of doses of beta -blockers administered in the past to patients with hyperadrenergic states, and a paucity of evidence of adverse outcomes (12). This would treat both SVT or sinus tachycardia. Later, he was found to have used cocaine.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered. Eur J Emerg Med.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
A middle aged male presented with chestpain. Birnbaum writes: "In patients with ACS without LVH, ST depression with negative T waves in the lateral leads is a sign of sub-endocardial ischemia and is an independent predictor of adverse outcome [11 – 13]. Here is his ECG ( Figure 1 ): What do you think? Baseline EKG, no MI.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. Studies show that 30% of NonSTEMI have an occluded infarct artery at the time of angiography done 24 hours after presentation. This patient had continued and ongoing pain. This is because of subtle ECG findings.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Gottlieb SO, et al.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
Sent by anonymous, edited by Pendell Meyers A man in his 50s with history only of hypertension presented with acute chestpain that started 45 minutes prior to presentation while doing yard work. Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardialinfarction, probably old."
Full case details and outcomes are below. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Repeat 0157 with ongoing chestpain: Basically the same features diagnostic of LAD occlusion. Physician: "No STEMI."
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 Annals of Emergency Medicine 2012;60:45-56. QRS V2 = 15.5
This is diagnostic of myocardialinfarction. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. She felt more comfortable being admitted. Int J Cardiol.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content