This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
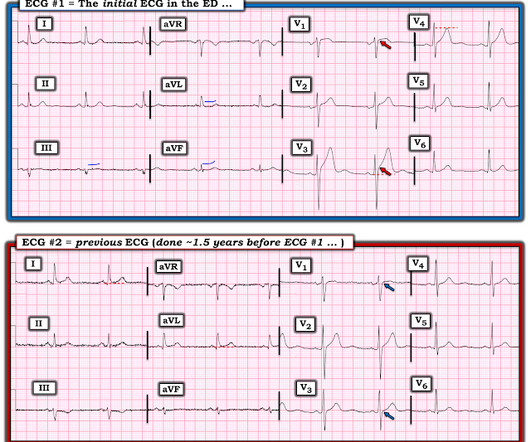
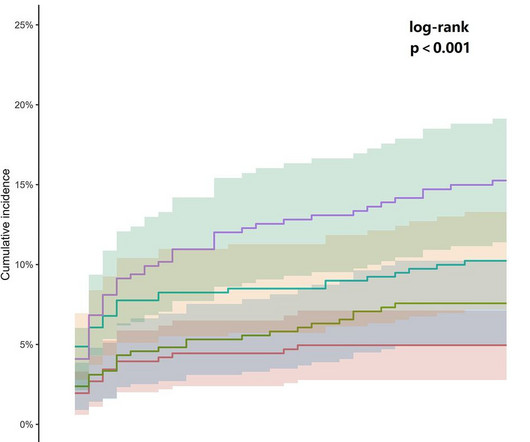
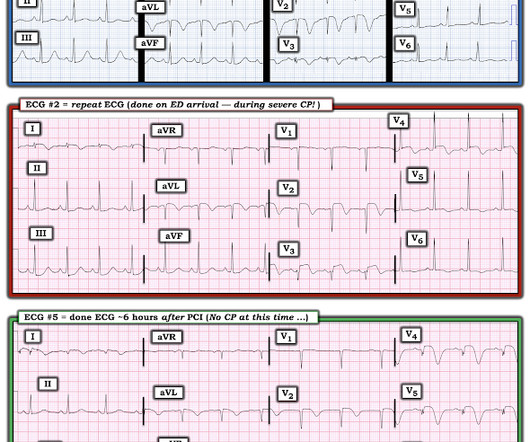
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
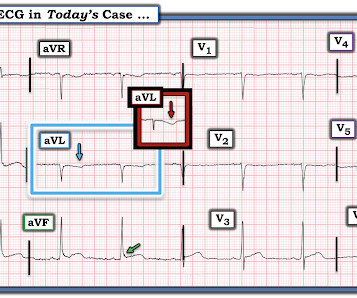
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chestpain as a “STEMI equivalent”[3] 3. ST depression in lead AVL differentiates inferior ST-elevation myocardialinfarction from pericarditis.
IntroductionAcute coronary syndrome refers to a group of diseases characterized by sudden, decreased blood supply to the heart muscle that results in cell death, also known as acute myocardialinfarction. The majority of patients (67.9%) have been diagnosed with ST- Elevated MyocardialInfarction and were classified as Killip class I.
I assumed it was a patient with acute chestpain. It was a man in his 30s with chestpain. Performance of Artificial Intelligence Powered ECG Analysis in Suspected ST-Segment Elevation MyocardialInfarction. This was sent to me from Sam Ghali ( @EM_Resus ) with no other information. What do you think, Steve?
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). A woman in her late 70s presented with left arm pain. The arm pain started the day prior when she was at the dentist's office for a root canal. See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG.
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. Sometimes posterior leads help, and sometimes they falsely reassure.
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. Always get serial ECGs in a patient with acute chestpain. It is constant, 9/10, left-sided CP that radiates into left arm and jaw.
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. It started while he was at rest after finishing a workout.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
Despite this, the patient went on to develop chestpain, which was accompanied by electrocardiographic signs of acute extensive anterior wall myocardialinfarction and elevated troponin I levels.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). The ECG is diagnostic of occlusion myocardialinfarction (OMI). All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
Written by Jesse McLaren A 65 year old with a history of atrial flutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chestpain, which was ongoing at triage. So a patient with high pretest probability (prior CABG with new chestpain), had new ECG changes showing posterior OMI.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Here is the ED ECG (a photo of the paper printout) What do you think?
A heart attack, or myocardialinfarction, happens when an artery becomes blocked, reducing blood flow to the heart muscle. Understanding the difference between heart attack and cardiac arrest can help in recognizing symptoms, seeking prompt medical care, and even saving lives. What is a Heart Attack?
Background Patients who experience acute myocardialinfarction (AMI) are at risk of recurrent AMI. Contemporary data on recurrent AMI and its association with return emergency department (ED) visits for chestpain are needed. Return ED visits for chestpain occurred in 27.0% (2017/7467) of index AMI survivors.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. In any case, it is diagnostic of OMI in a chestpain patient. But there is also perhaps some STD in inferior leads -- this would support LAD.
Background Despite the crucial role of Chestpain centers (CPCs) in acute myocardialinfarction (AMI) management, China's mortality rate for ST-segment elevation myocardialinfarction (STEMI) has remained stagnant.
A 60-something male presented stating that he had had chestpain that morning which awoke him from sleep but then resolved after several minutes. He has had similar pain in the past which he attributed to acid reflux. He is pain free now. The patient is pain free at the time of this ECG: What do you think?
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
A 29 year old male presented with 6 hours of stuttering chestpain, constant for the last hour, worse with breathing. Take home point here : Obtain an ECG on anyone with chestpain. Appearance of abnormal Q-waves early in the course of acute myocardialinfarction: implications for efficacy of thrmoblytic therapy.
A 50-something man presented in shock with severe chestpain. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. The patient was in clinical shock with a lactate of 8.
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
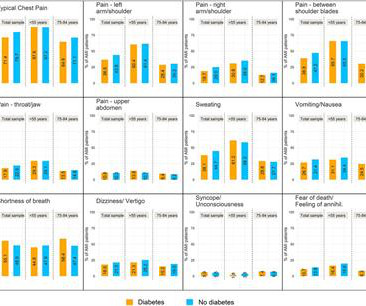
Background The objective of this study was to investigate the differences in presenting symptoms between patients with and without diabetes being diagnosed with an acute myocardialinfarction (AMI). Results Patients with diabetes had significantly less frequent typical pain symptoms, including typical chestpain.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chestpain remains unclarified.
For life-threatening events involving complete occlusion of a coronary artery, the activation of ST-elevation myocardialinfarction protocols instructs the emergency services to provide immediate treatment and liaise directly with cardiac centres regarding invasive management, in turn, reducing morbidity and saving lives.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? Pol Arch Intern Med. 2017;127:401–411. Circulation.
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
(Unusual and puzzling, as there was a large focal acute MI) Final Diagnosis: Acute MI, Non ST Elevation MyocardialInfarction. The presence or absence of ST Elevation is a poor marker with which to describe a myocardialinfarction. = NSTEMI is extremely heterogenous, from a very tiny Non-OMI to a massive OMI.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. See this article by Widimsky: Primary angioplasty in acute myocardialinfarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy [link]
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. Electrocardiographic Manifestations: Acute posterior wall myocardialinfarction. Posterior myocardialinfarction: the dark side of the moon. This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! J Emerg Med 2001; 20:391-401.
But syncope or seizure alone, without chestpain, is not enough to call it Wellens syndrome. Without chestpain, the pretest probability is not very high. Further review of systems with the patient fully awake revealed that the patient had been having chestpain on and off all week. It can be much lower.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Why is there this notion that myocardialinfarction cannot be diagnosed in the setting of ventricular paced rhythm?
Written by Pendell Meyers A middle aged man called EMS for acute chestpain. Physician accuracy in interpreting potential ST-segment elevation myocardialinfarction electrocardiograms. EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I said "Not OMI.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardialinfarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6. What do you think?
Background Diagnosis and prognostic evaluation of acute myocardialinfarction (AMI) are crucial for patients. Methods The study subjects were 90 AMI patients and 50 acute chestpain patients (control). All patients were examined by echocardiography and recorded LVEDV, LVESV, and LVEF.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. Pseudo ventricular hypertrophy and pseudo myocardialinfarction in Wolff-Parkinson-White syndrome. What do you think? Khan and Shaw.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardialinfarction. Who needs the cath lab? Int J Cardiol Heart Vasc 2021 2. Aslanger et al. Lemkes et al.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." References Lobo AS et al. JACC 2019 Sep 10;74(10):1290-1300.
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardialinfarction of any kind.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content