This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. NOTE #1: Sinus tachycardia is not usually seen in an uncomplicated acute MI.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. With normal EF the tachycardia is not compensatory.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Just as important is pretest probability: did the patient report chestpain prior to collapse?
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
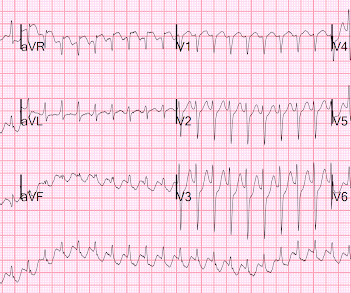
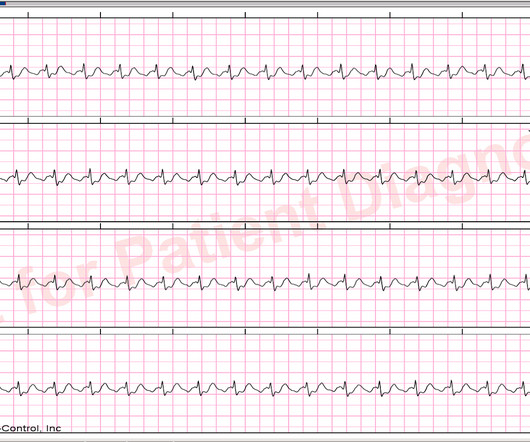
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. The ECG below was recorded.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. They agreed ischemia was likely in the setting of demand given DKA and infection.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The ECG was incorrectly interpreted as no signs of ischemia. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. His vitals were within normal limits.
Only 5-13% of patients with chestpain and LBBB have MI; many fewer have coronary occlusion. Whenever you see tachycardia with bundle branch block, you should suspect that it is rate related BBB. After resolution, there was T-wave inversion in V1-V3, highly suggestive of ischemia. link] Shvilkin et al.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". He mentioned "cancer" and "chest". There is a narrow complex tachycardia at a rate of 130. He was awake, with a pulse of 130 and BP of 50/30. Is is sinus?
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? She had a very elevated troponin T at 12,335 ng/L at the time of presentation. The patient in today’s case suddenly became tachycardic while sleeping.
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. More detailed reviews of subendocardial ischemia, as well as acute ECG patterns that breach the typical presentation, can be found here: [link] [link] Imaging revealed no acute head, or spinal, injuries.
40-something yo who is on flecainide and diltiazem had sudden onset chestpain, palpitations, shortness of breath and diaphoresis : Rate is 220. It is a regular narrow complex tachycardia. There is a lot of ST depression -- this is ischemia caused by the very fast rate and is an indication for emergent electrical cardioversion.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. He had this ECG recorded. Are the lungs clear?
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia.
A male in his 60's called 911 for dizziness and chestpain, onset with exertion. Here is his initial rhythm strip (it is not a full 10 seconds): Wide complex tachycardia, rate 235 This is a very wide complex regular tachycardia at a rate of 235. It should be considered to be Ventricular Tachycardia and treated as such.
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chestpain. Chestpain was resolved upon arrival in the ED. Is there ischemia? A repeat ECG had sinus rhythm at a rate of 54 and normal conduction (no LBBB), and was completely normal with no ischemia. What is it?
The chestpain quickly subsided. The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. Are you worried about OMI in this case? His response was: "I would not call it OMI.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. What is the rhythm?
NOTE: It's important to correlate ongoing circumstances at the time that a prior tracing was done ( ie, Was the patient stable and asymptomatic — or were they having chestpain, an exacerbation of heart failure, or some other ongoing process at the time the prior ECG was recorded? ).
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. If a patient presents with chestpain and a normal heart rate, or with shockable cardiac arrest, then ischemic appearing ST elevation is STEMI until proven otherwise.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? ST depression. Myocardial Contusion?
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. The patient had none of these conditions. It was stented.
This is the prehospital ECG from an 81 year old man with acute chestpain. The problem is, that the PR interval of the upright deflection in lead II ( under the RED arrows ) is relatively long ( clearly more than 1 large box in duration ) — and if anything, the PR interval should shorten when there is tachycardia. Arrhythmia?
Advanced cardiac imaging especially in atypical presentations, can aid in early diagnosis.Case:A 59 year-old man with history of biopsy-proven pulmonary sarcoidosis presented with non exertional chestpain for 2 months. Stress echocardiogram ruled out myocardial ischemia.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
The presenting complaint was chestpain — and the patient collapsed soon after arrival in the ED. The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. It should be known that each category can easily manifest the generic subendocardial ischemia pattern.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? In addition to sinus tachycardia, the only abnormalities listed by the computer were "low voltage, precordial leads" and "anteroseptal infarct, old.Q Physician: "No STEMI."
Case 1 A middle aged woman presented with acute chestpain and shortness of breath, unclear time since onset, and likely with episodic symptoms off and on throughout the day. That first ECG (the one at the top) was interpreted as "no evidence of ischemia." Submitted by anonymous, written by Pendell Meyers.
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Now the patient is in sinus tachycardia. Her initial EKG is below. Same as initial ECG.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( The other main consideration — is to take another look at the 12-lead ECG, and assess this for recent ischemia or infarction. How would YOU interpret the ECG in Figure-1 ?
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y. Hypokalemia c.
A recent similar case: A 40-something with chestpain. A useful classification of WCT ( W ide- C omplex T achycardia ) rhythms — separates them into those that are mono morphic ( with similar QRS morphology during the tachycardia ) vs those that are poly morphic ( in which QRS morphology varies ). Acute ischemia?
ie, with syncope-presyncope, fatigue, dyspnea, chestpain? ). Ruling out other potential causes of bradycardia ( ie, recent ischemia-infarction; hypothyroidism ). 2 short runs of SVT ( presumably atrial tachycardia ). 2 short runs of SVT ( presumably atrial tachycardia ). No pause beyond 2.0 No pause beyond 2.0
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content