This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. This confirms that the pain was ischemia and is now resovled. Because the pathologist determines the degree of stenosis by dividing the lumen area by the total area, the degree of stenosis will be overestimated.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
In a 57-year-old man with chestpain, an ECG obtained by EMS showed widespread ST-segment depressions. At the hospital, left main coronary-artery stenosis was seen on angiography (shown in a video).
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
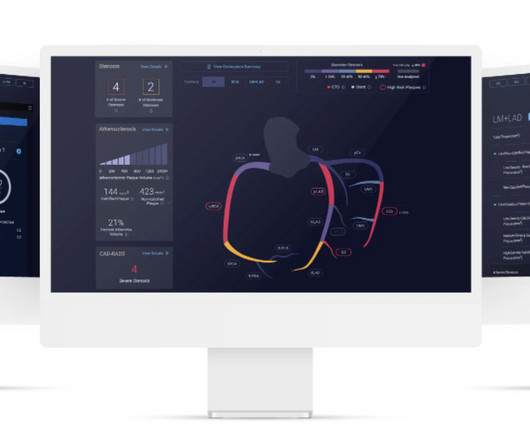
The study describes the validation of Cleerly's artificial intelligence-guided quantitative coronary CT angiography (AI-QCT) ISCHEMIA technology for diagnostic accuracy and prognostic risk stratification. High Diagnostic Accuracy of AI-ISCHEMIA in Comparison to PET, FFR-CT, SPECT, and Invasive FFR: A Pacific Substudy. 2024.01.007.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. More detailed reviews of subendocardial ischemia, as well as acute ECG patterns that breach the typical presentation, can be found here: [link] [link] Imaging revealed no acute head, or spinal, injuries.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. 2 years prior he had an angiogram which showed 90% proximal stenosis of the circumflex. The pain did not resolve with NTG, and so he went to emergent angiography: 1. Left main: no obvious stenosis.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 2024, [link].
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. Here is the history: A 40-something male had intermittent chest discomfort until 90 minutes prior to presentation, when it became constant. At 100 minutes, the above ECG was recorded.
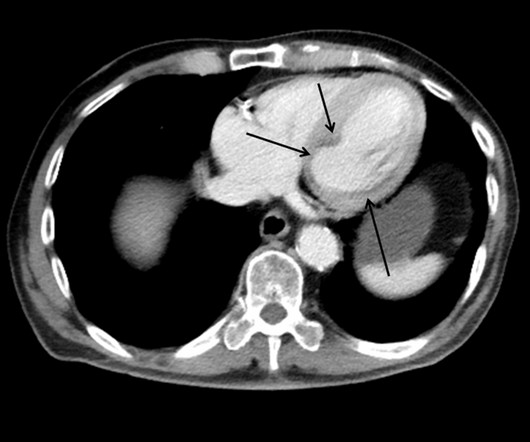
This case shows a CT image of subendocardial ischemia. This patient presented with a mechanical fall and had chestpain. His chestpain increased and this ECG was recorded: Now there is increasing inferior ST elevation. Severe Left Main disease, and chestpain with contrast injection into the LM.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. Is this Acute Ischemia? More on LVH.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chestpain and diaphoresis, which recurred two hours prior to presentation. The chestpain was refractory to nitro so the cath lab was activated: 100% proximal LAD and 99% mid circumflex occlusions.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Pericarditis would be even more unlikely in someone without chestpain. Chestpain is squeezing or tight in nature.
The patient’s chestpain spontaneously resolved before he was evaluated and has a repeat ECG obtained at 22:12 obtained shown below. In context, of course, it is clear that the patient is reperfusing, as pain has dissipated and the diagnostic findings of OMI have become more nonspecific. This ECG is more difficult.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
A 60-something awoke with 10/10 crushing chestpain. I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. He walked in to triage.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. Below is a still image with the red arrow indicating the subtotal LMCA stenosis. What do you think?
This is ischemia until proven otherwise. Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. I learned that the patient is on Sotalol for control of PVCs. This explains the long QT.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
An ECG was recorded during pain: What do you think? This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. These suggest inferior OMI with possible RV involvement. with ADDED STE in III?
A middle aged man had off and on chestpain for 2 weeks, then 2 hours of more severe and constant pain. Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Ischemia may be so brief that Wellens' waves do not evolve 3. Lessons: 1.
(In other words, the artery was occluded but has sponteneously reperfused, resulting in pain relief) It is important to monitor patients with Wellens' syndrome for re-occlusion, which is usually, but not always, associated with recurrent chestpain. The patient remained pain free. Learning Points: 1.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Angiography revealed a 30% nonobstructive stenosis of the mid LAD.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Angiography : LMCA — 90-99% osteal stenosis. The below ECG was recorded.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. The data is overwhelming every way you can possibly look at it. years of age versus 59.0±8.4
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. It should be known that each category can easily manifest the generic subendocardial ischemia pattern.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
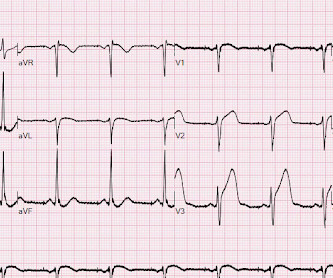
Case A 47 year old male called 911 for severe chestpain. Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. This ECG is diagnostic of ischemia.
There is normal R-wave progression in the precordial leads with no evidence of ischemia. COPD, Idiopathic PAH, acute or chronic PE, pulmonary valve stenosis, etc) 3) Conditions affecting RV myocardial contractility, such as ARVD or RV infarction The ECGs does not really show any signs of chronic RV dilation or hypertrophy.
Hiding behind the technicalities PCI demands reduction in percentage stenosis , resulting in pre-defined minimal luminal area (MLA), maximizing net luminal gain, & restoration of TIMI 3 flow in all three coronary arteries.These are the popular scientific parameters. Please note ORBITA -2 is not an antidote to ORBITA-1) ,Read this 1.AVERT
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Here is his triage ECG: What do you think? The ECG was interpreted as non-ischemic.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
Case 1 A middle aged woman presented with acute chestpain and shortness of breath, unclear time since onset, and likely with episodic symptoms off and on throughout the day. That first ECG (the one at the top) was interpreted as "no evidence of ischemia." Another lesion in the proximal LAD with 80% stenosis was stented as well.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content