This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
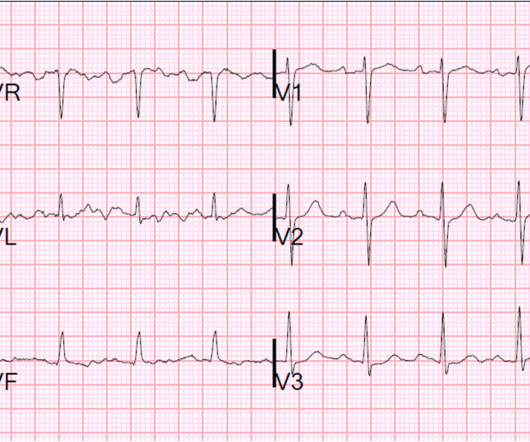
By Magnus Nossen This ECG is from a young man with no riskfactors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG?
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. It started while he was at rest after finishing a workout.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
A 20-something male presented from an outside facility with Chestpain. No thromboembolism risks, not pleuritic, no radiation to the back. No cardiac riskfactors, no cocaine use. T-wave inversion in V2 is inconsistent with early repol, and is typical of posterior ischemia. Vital signs were normal.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
A 39 yo otherwise healthy man with no riskfactors was walking at the mall when he developed chest pressure. Thus, there are some suspicious abnormalities, but no definite signs of ischemia. The difference is significant and highly suggests posterior ischemia. He was diaphoretic. It is very subtle but real.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
A male in his 60's called 911 for chestpain. He had some cardiac riskfactors including hypertension, on meds, but no previous coronary disease. His pain was intermittent and he was vague about when it was present and when it was resolved. Is it subendocardial ischemia, or inferior MI?
This case was recently posted by Tyron Maartens on Facebook EKG club (he agreed to let me post it here), with the following clinical information: "42 year old male with two weeks of intermittent chest discomfort, awoke 4 hours prior to this ECG with a more severe, heavy chestpain (5/10). BP 112/80, SpO2 100%.
She did not report any chestpain or pressure. She was brought to the Emergency Department and this ECG was recorded while she was still feeling nauseous but denied chestpain, shortness of breath, or other symptoms: What do you think? The morphology of STE is not diagnostic of being due to acute transmural ischemia.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. It should be known that each category can easily manifest the generic subendocardial ischemia pattern.
Written by Pendell Meyers A male in his early 50s presented with waxing and waning chestpain starting at rest. He had multiple cardiovascular riskfactors and the EM physician strongly suspected ACS. Here is his initial ECG: What do you think? mm of the "required" 1.0 Repeat ECGs are almost always helpful.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
hours of substernal chest pressure. She had zero CAD riskfactors. About this time, the 4th troponin, drawn at 8 hours after onset of pain, peaked at 20.956 ng/mL. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
The patient contacted EMS after a few hours of chestpain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder. The chestpain was described as both sharp and pressure like. There is slight ST depression in lateral chest leads V4,V5,V6 — but I thought this to be nonspecific.
A 40 something woman with a history of hyperlipidemia and additional riskfactors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". The source of this case is anonymous.
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. RiskFactors: High Cholesterol. Smith and Meyers have emphasized on many occasions — ST depression that is maximal between leads V2-to-V4 in a patient with new chestpain should be assumed to be posterior OMI until proven otherwise.
Denied headache, chestpain, nausea / vomiting. No history, meds, or riskfactors. If this patient had chestpain and the value suggested early repol, I would be very hesitant to act on it. They gave him water with salt, as he thought he was dehydrated." Ambulated to ambulance for eval. Wang, page 171).
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. He has no cardiovascular riskfactors except smoking for 10 pack-years. Here are his publications.) His ECG is shown below.
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. To quote Dr. Stephen Smith: "The worst riskfactor for a bad outcome in acute MI is young age."
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Pain largely resolved prior to EMS arrival but completely subsided after prehospital NTG and aspirin. Triage EKG: What do you think?
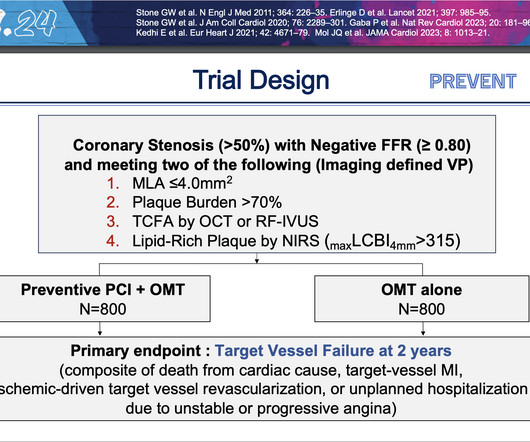
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood. The study was funded by Cardiovascular Research Foundation, Abbott, Yuhan Corp, CAH-Cordis, Philips and Infraredx, a Nipro company.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Women also had more cardiovascular riskfactors, including hypertension (66.6%
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
Ischemia Trial In an attempt to clarify this question, a similar trial was done called the Ischemia Trial, which had important differences to the Courage trial but again tried to answer a similar question 3. But what about those with symptoms such as chestpain or shortness of breath as a result of their coronary artery disease?
A late middle-aged man presented with one hour of chestpain. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. Left BBB vi. Pathologic Q-waves viii.
Since he was recovering from a recent bout of Influenza-like illness and said yes to several ILI screening questions at triage, his chest tightness and diaphoresis were initially attributed to this. The patient has acute persistent refrectory chestpain and elevated troponin. There is no need for another ECG.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a riskfactor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. Improved chestpain is unresolved chestpain.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." The presenting complaint noted at Triage was, "a 50yo man with chestpain!" Ischemia or infarction.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content