This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. Circulation Research , 56 (2), 184–194. Is there STEMI? What is the rhythm?
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Pericarditis would be even more unlikely in someone without chestpain. Chestpain is squeezing or tight in nature.
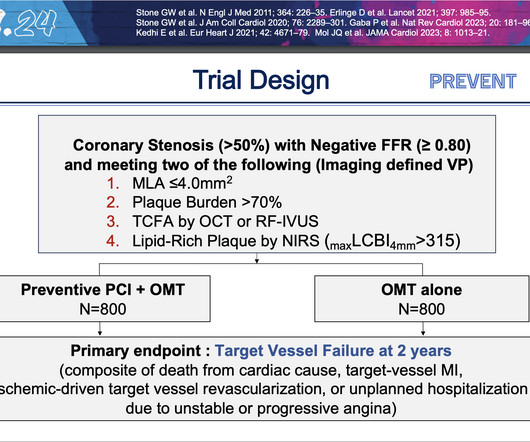
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood. To test this strategy, researchers enrolled 1,606 patients treated for coronary artery disease at 15 centers in four countries.
Dr. Yang is also winner of the SCCT Best Abstract Award for his submission, “Coronary CT Angiography-derived Precursors Of Acute Coronary Syndrome In Ischemia-causing Lesions.” The SCCT Best Abstract Award is supported by the Cardiovascular Research Foundation of Southern California (CVRF of So.
Patients with coronary artery diseaseplaque buildup inside the arteries that leads to chestpain, shortness of breath, and heart attackoften undergo PCI, a non-surgical procedure in which interventional cardiologists use a catheter to place stents in the blocked coronary arteries to restore blood flow.
ObjectiveA significant proportion (85%) of low-risk non-ST-elevation acute coronary syndrome (NSTE-ACS) patients do not receive objective confirmation of ischemia by stress echocardiography (SE), yet remain a healthcare burden due to lower long-term survival and overuse of medical services.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. Cardiology aware.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death.
Because of the clinical and medicolegal consequences of incorrectly discharging an MI patient, medical practices and clinical research have largely focused on addressing MI underdiagnosis. One study revealed that a quarter of all ED visitors underwent a troponin test, even though less than half of them had chestpain.
Five highly-anticipated late-breaking clinical trial sessions, an ACC/AHA guidelines update session and a host of featured clinical research sessions have been announced by program planners for the American College of Cardiology’s 73 rd Annual Scientific Session & Expo to be held April 6-8 in Atlanta, GA.
A 40-something male with no previous cardiac disease presented with chestpain. Here is his ECG: There is no clear evidence of OMI or ischemia. Moreover, the research which appears to confirm this idea was indeed in relation to the circumflex, but they did not study Occlusion ; rather, they studied asymptomatic coronary disease.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
Ischemia Trial In an attempt to clarify this question, a similar trial was done called the Ischemia Trial, which had important differences to the Courage trial but again tried to answer a similar question 3. But what about those with symptoms such as chestpain or shortness of breath as a result of their coronary artery disease?
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
About this time, the 4th troponin, drawn at 8 hours after onset of pain, peaked at 20.956 ng/mL. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. She has done quite a bit of research on the topic.
Case An elderly patient had acute chestpain and 911 was called. And, in cases like the elderly patient with new-onset chestpain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. It is important for cardiologists to realize that a paramedic may see something they do not.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Whether stenting a narrowed coronary artery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. Subscribe now 1 ISCHEMIAResearch Group. However, the devil is in the detail when considering this question, and I have discussed it in more detail here. What About Symptoms?
I do research on Cardiologs' algorithm: Smith SW et al. But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. The Ratios of STE to S-wave: V1: 2.5/16
I remember Allie well from her days in the Research volunteer program at Hennepin. It was from a patient with chestpain: Note the obvious Brugada pattern. This was submitted by Alexandra Schick. Dr. Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island. The article is edited by Smith.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chestpain that feels like heartburn but that radiates to the left arm. See this other post: Chestpain, a ‘normal ECG’ a ‘normal trop’, and low HEART and EDACS score: discharge home? Below is the ECG.
In a study published by the American Heart Association, “Sex and Age Differences in the Association of Depression With Obstructive Coronary Artery Disease and Adverse Cardiovascular Events,” researchers investigated 3,237 patients (35% women) undergoing coronary angiography to evaluate for coronary artery disease (CAD).
As to ST-T wave changes in the 12-lead ECG — although some leads show T wave inversion (ie, in leads III, V3 and V4 ) — I did not think this looked acute in this 30-year old man without chestpain. No evidence of ischemia. Figure-2: I’ve labeled atrial activity from Figure-1 with colored arrows. What about the Repeat ECG?
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. Left BBB vi. Pathologic Q-waves viii.
SPECT continues to be a first-line test to diagnose coronary ischemia, often instead of or before invasive coronary angiography. To determine if AI-CCTA could hold its own, researchers analyzed CCTA images from 175 patients using Cleerlys AI-QCT ISCHEMIA model and found it outperformed SPECT when compared to invasive angiography.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. link] Bentzon, J.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content