This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. million patients in the United States.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. Here is the history: A 40-something male had intermittent chest discomfort until 90 minutes prior to presentation, when it became constant. At 100 minutes, the above ECG was recorded.
There is also STE in lead III with reciprocal depression in aVL and I, as well as some subendocardial ischemia pattern with STD in V5-V6 and STE in aVR. Aslanger's is a combination of acute inferior OMI plus subendocardial ischemia, and due to the ischemia vectors , it has STE only in lead III. Moreover, there is tachycardia.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. Xray was consistent with pulmonary vascular congestion. 40 mg of furosemide was given.
This is a previously healthy male teenager who was awoken by chestpain. He was seen at another hospital and found to have a slightly elevated troponin, then underwent a CT pulmonary angiogram (PE) protocol which revealed a right sided pneumonia. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. Only 5-13% of patients with chestpain and LBBB have MI; many fewer have coronary occlusion. Moreover, and importantly, there was sinus tach.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
He then went on to say: "40-something with chestpain for one hour. Burning pain subxiphoid and into throat." It does not usually represent subendocardial ischemia, but rather it is usually reciprocal ST depression, reciprocal to inferior ST elevation. Had episode of nausea and dizziness when it started.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. More detailed reviews of subendocardial ischemia, as well as acute ECG patterns that breach the typical presentation, can be found here: [link] [link] Imaging revealed no acute head, or spinal, injuries.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) An 80-something woman who presented with chestpain and dyspnea.
An ECG was recorded during pain: What do you think? This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. These suggest inferior OMI with possible RV involvement. with ADDED STE in III?
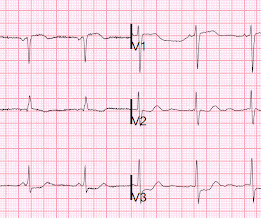
There is normal R-wave progression in the precordial leads with no evidence of ischemia. large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. Any cause of pulmonary hypertension. What do you think?
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. He was awake, with a pulse of 130 and BP of 50/30. Fluids were started.
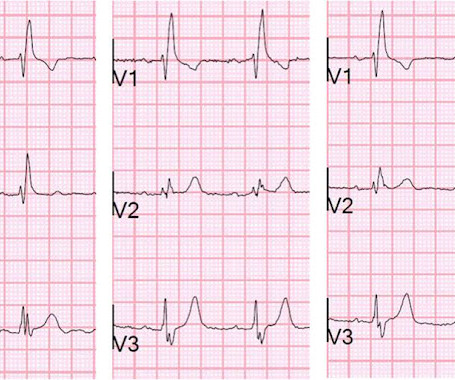
56 y/o male who presented with 12/10 severe chestpain starting at 3AM, radiating to his upper back. He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different. Here are V1-V3 from the last 3 ECGs: It is now clear that there is cardiac ischemia. Wraparound?
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed.
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chestpain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. A chest X-ray was obtained: This was read by radiology as "Bilateral lower lobe interstitial opacities.
Advanced cardiac imaging especially in atypical presentations, can aid in early diagnosis.Case:A 59 year-old man with history of biopsy-proven pulmonary sarcoidosis presented with non exertional chestpain for 2 months. Stress echocardiogram ruled out myocardial ischemia.
A 52 year old woman presented with chestpain. There was some pulmonary edema. This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. They texted me the following ECGs, which I viewed in the shade of a pine tree on a glorious sunny snowy landscape.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? ST depression. Myocardial Contusion?
Then the notes mention "cardiogenic shock" but without any reference to a cardiac echo or to a chest x-ray. Was there pulmonary edema? Now chestpain free. Furthermore, there are T-wave changes in V2 and V3 which are highly suggestive of ischemia, but difficult to localize: anterior? right ventricular?
If a patient presents with chestpain and a normal heart rate, or with shockable cardiac arrest, then ischemic appearing ST elevation is STEMI until proven otherwise. The estimated pulmonary artery systolic pressure is 37 mmHg + RA pressure. Normal estimated left ventricular ejection fraction lower limits of normal.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. She was noted to be tachycardic and her heart sounds were distant on physical exam.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity. Which is true.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. Then there is the significant ST elevation we see in lead V1.
From there, the right ventricle pumps the blood to the lungs via the pulmonary arteries for reoxygenation. Additionally, the heart’s high demand for oxygen makes it particularly vulnerable to conditions like ischemia (reduced blood flow), which can weaken or damage the heart muscle if left untreated.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
A late middle-aged man presented with one hour of chestpain. Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. I have read articles that say that patients without ischemia are at low risk of complications from hypokalemia, But it is not entirely without risk.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. Left BBB vi. Pathologic Q-waves viii.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
A 50-something man presented with worsening severe exertional chestpain which was just resolving as he had an ECG recorded in triage. Watch what happends as the heart recovers from its episode of ischemia. The ECG shows inferior ischemia. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know?
He denied chestpain. Bedside POCUS showed very poor LV function and a few pulmonary B lines. A Chest X-ray did not show pulmonary edema. Time 7 hours lead reversal There is limb lead reversal (QRS in I and aVL are now inverted), but nevertheless one can see that the ischemia appears to have resolved.
These ECGs were texted to me by one of our previous ultrasound fellows, Will Smoot An elderly male arrived via EMS for acute substernal chestpain with radiation to left shoulder and arm that awakened him from sleep at 0030. The pain was relieved by one prehospital NTG spray. No prior similar symptoms or known CAD.
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. He presented to the emergency department for evaluation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content