This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque.
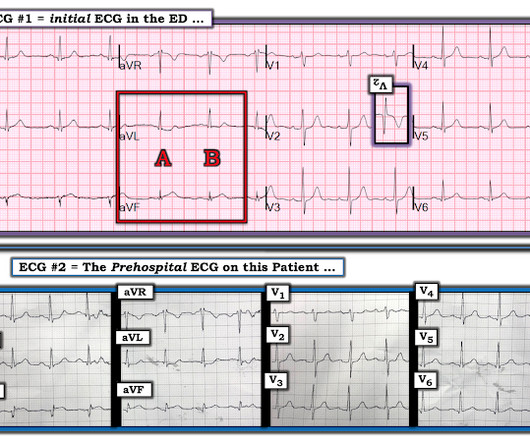
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This strongly suggests reperfusing RCA ischemia.
First runner-up for the YIA is Seokhun Yang, MD , of Seoul National University Hospital, for his abstract, “Prognostic Implications Of Coronary CT Angiography-derived Plaque And Hemodynamic Features On Acute Coronary Syndrome Across Varying Time Intervals: Emerald-ii Study.” and the Ma Family, who provided a $5,000 case prize for the winner.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. Is this Acute Ischemia? More on LVH.
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. More detailed reviews of subendocardial ischemia, as well as acute ECG patterns that breach the typical presentation, can be found here: [link] [link] Imaging revealed no acute head, or spinal, injuries.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. For now she can only say Not OMI.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
An ECG was recorded during pain: What do you think? This suggests diffuse subendocardial ischemia. However, along with that subendocardial ischemia, there is also STE in lead III with reciprocal ST depression in aVL, and some STE in V1. These suggest inferior OMI with possible RV involvement. with ADDED STE in III?
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). He had no further chestpain.
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. 2021 ACC/AHA ChestPain Guidelines.
However ,we have some effective clinical and pathological markers too, for effective re-vascularisation They are clinical well being and good functional capacity , relief from chest-pain, reduction of plaque volume, plaque stabilisation, maintenance of collaterals , microvascular patency , reduction of recurrent events.
Here is a case of an 89 year old woman who had syncope but no chestpain or shortness of breath. She is diagnosed with "demand ischemia" and discharged home. (#2) She had the following EKG at 0700 : (#3) Here there is 4 mm of ST elevation that can only be due to myocardial ischemia. She has a troponin of 0.13
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. It should be known that each category can easily manifest the generic subendocardial ischemia pattern.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
About this time, the 4th troponin, drawn at 8 hours after onset of pain, peaked at 20.956 ng/mL. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. Again, cath lab was not activated.
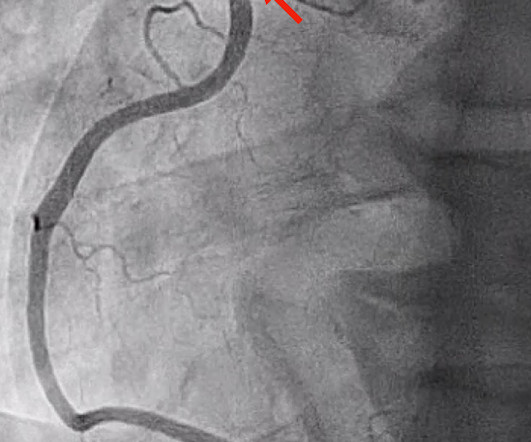
A 40-something woman had sudden chestpain. Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. She called 911. But which myocardial walls are affected?
A recent similar case: A 40-something with chestpain. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Is this inferior MI? Just as interesting is EKG 1, 24 minutes before the first: What do you think here?
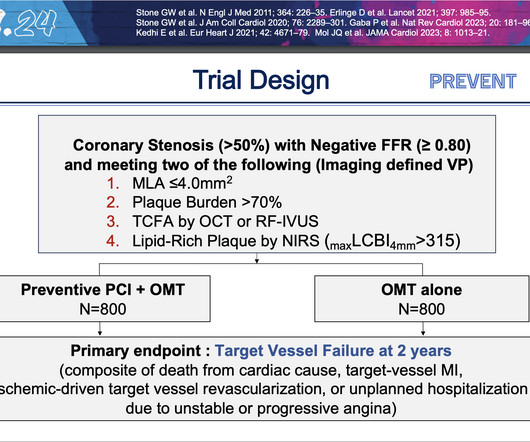
PCI is commonly used to open blocked arteries to treat significant myocardial ischemia , which occurs when the heart muscle does not get enough oxygenated blood. These findings demonstrate that the focal treatment of high-risk vulnerable plaques may improve patient prognosis beyond optimal medical therapy alone.”
This was interpreted by the treating clinicians as not showing any evidence of ischemia. He did not remember whether he had experienced any chestpain. He was intubated in the field and sedated upon arrival at the hospital. Here is his presenting ECG: ECG 1, t = 0 What do you think? He was admitted to cardiology.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 2024, [link]. 22, 30 Nov.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness.
Coronary Artery Disease (CAD) CAD, which involves the narrowing or blockage of coronary arteries due to plaque buildup, can reduce blood flow to the heart. This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Patients with coronary artery diseaseplaque buildup inside the arteries that leads to chestpain, shortness of breath, and heart attackoften undergo PCI, a non-surgical procedure in which interventional cardiologists use a catheter to place stents in the blocked coronary arteries to restore blood flow.
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chestpain (angina) or, in more severe cases, a heart attack. CAD is one of the leading causes of heart attacks.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chestpain associated with shortness of breath for the last 2 days. This was her ECG (it is unclear if this was with or without pain): Computerized ECG Read: “Normal sinus rhythm. This case was written by Sam Ghali: ( @EM_RESUS ). Normal ECG.”
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. Heart health is vital for us, and it is essential to keep track of it.
Arteries generally narrow and occlude for one of two reasons: The progressive accumulation of plaque. A plaque ruptures, and a clot forms in the artery, thereby occluding it. There are the ‘garden variety’ heart attacks whereby a plaque ruptures in the coronary artery, called a spontaneous heart attack. N Engl J Med.
Whether stenting a narrowed coronary artery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. The cause of angina usually involves inadequate blood flow reaching the heart muscle because of significant narrowing of the artery due to plaque buildup. What About Symptoms?
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. As there was ruptured plaque, this is NOT Prinzmetal's angina. Values: STE60V3 = 2.0, There was good flow.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Lead V2 shows RR’ QRS configuration, and although ST depression is otherwise expected here, the discordance is a bit excessive.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
Influenza-like illness can also trigger plaque rupture. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L. The patient has acute persistent refrectory chestpain and elevated troponin. Just go to the cath lab!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content