This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
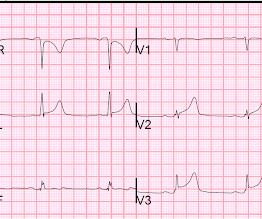
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. But are there any other signs of Occlusion MI? Kontos et al. J Am Coll Cardiol 2022 4.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. It is easy to say pericarditis in such a case.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. Pericarditis maybe." Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. Meyers' words — "is one of the rare ECGs that is actually specific for pericarditis".
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). As already mentioned, this patient could have post-infarction regional pericarditis from a large completed MI. Sinus tachycardia has many potential causes. Hammill SC.
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
A young otherwise healthy man presented with 4 hours of sharp 10/10 substernal chestpain. But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. This is a good sign for myocardial infarction and does not happen in pericarditis. BP was 160.
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". Clinician and EKG machine read of acute pericarditis.
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. What do you think?
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. Ischemic ST depression includes posterior OMI and subendocardial ischemia.
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Pericarditis would be even more unlikely in someone without chestpain. Chestpain is squeezing or tight in nature.
There is also STE in lead III with reciprocal depression in aVL and I, as well as some subendocardial ischemia pattern with STD in V5-V6 and STE in aVR. Aslanger's is a combination of acute inferior OMI plus subendocardial ischemia, and due to the ischemia vectors , it has STE only in lead III. Moreover, there is tachycardia.
3 hours prior to calling 911 he developed typical chestpain. This rules out pericarditis, which essentially never has reciprocal ST depression. When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia. This is not pericarditis because: a.
More Smith comment: it is true that ST depression (STD) due to subendocardial ischemia does not localize [it is usually diffuse ST depression, in multiple leads and not reciprocal to ST elevation in an opposite territory], this ST depression is different! Notice how useful serial ECGs are! mm ST depression in aVL. mm ST depression in aVL.
You do NOT see this in normal variant STE, nor in pericarditis. The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI.
Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Weren't you taught that "new tall T wave in V1" is concerning for ischemia, and so this is the opposite? Expert ECG interpretation can often distinguish normal variant STE from OMI from pericarditis.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? ST depression. Myocardial Contusion?
He denied fevers and chills, abdominal pain, chestpain, or SOB. Normal RBBB, no evidence of ischemia. Patients with completed, transmural infarct are also at risk for post-infarction regional pericarditis and myocardial rupture. Patient stated his dry weight is around 85 kg. He did have one episode of diarrhea.
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. Pericarditis? A straight ST segment virtually never happens in inferior ST elevation that is NOT due to OMI (normal variant, pericarditis) 4. More likely, these T waves probably reflect ischemia of uncertain age.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? The second most common cause of medical cardiac tamponade is acute idiopathic pericarditis. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia.
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. STEP #2 = Clinical Impression — in which we correlate our assessment that we made in Step #1 to the clinical situation at hand.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. ST depression. Myocardial Contusion?
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
All of the patients presented with chestpain , and they are all in triage. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. True Positive ECG#2 : Also sinus rhythm.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 More likely, the patient had crescendo angina, with REVERSIBLE ischemia for 48 hours that only became potentially irreversible (STEMI) at that point in time. Myocardial Rupture and Postinfarction Pericarditis.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chestpain, dyspnea and weakness on the treadmill. In the ED he had some continued chestpain and hypotension. Myocardial rupture is usually preceded by postinfarction regional pericarditis (PIRP).
A 26 year old male presented with syncope and chestpain. No signs of OMI" The chestpain resolved after some time, and another ECG was recorded: The ST Elevation is nearly gone. Doesn't this necessarily mean that he was having ischemia? This appears to be an inferior OMI What do you think? She is very good.
However, with widespread ST depression, this could also be due to diffuse subendocardial ischemia. Everything is complicated by the arrest and hypotension: Is the ischemia caused by the instability, or the instability caused by the ischemia? Myocardial rupture is usually preceded by postinfarction regional pericarditis (PIRP).
Scenario 1 : The patient presents with 24 hours of substernal chestpain. The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves.
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. A 30-something woman with chestpain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chestpain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content