This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
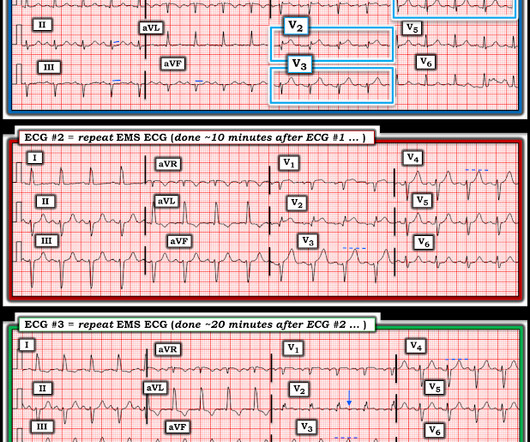
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
Written by Jesse McLaren A 65 year old with a history of atrial flutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chestpain, which was ongoing at triage. The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. What do you think?
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. link] ] Outcome The patient emerged neurologically intact.
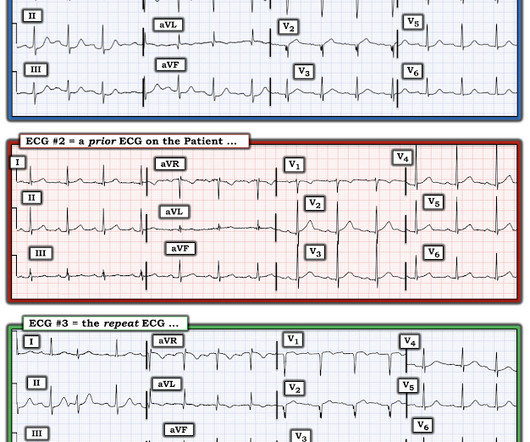
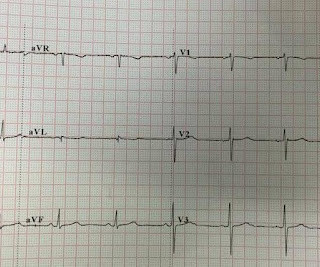
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
A 41-year-old male who presents to the emergency department with chestpain. Patient reports approximately 2 hours prior to arrival he developed a sharp chestpain that radiates into his left arm and left lower leg. Describes the radiating pain as numbness/tingling. No shortness of breath. No recent travel.
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
Written by Jesse McLaren Four patients presented with chestpain. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This strongly suggests reperfusing RCA ischemia. Lobo et al.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. The ECG does not show any definite signs of ischemia. The below ECG was recorded.
A middle aged male presented with chestpain. There may be ischemia present, but it is not evident on the ECG. In LVH, T-wave inversions are usually much more assymetric , like these (Figure 2): Acute Chestpain, but baseline ECG. Here is his ECG ( Figure 1 ): What do you think? All troponins were negative.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. Neth Heart J.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
Submitted by Dr. Dennis Cho (@DennisCho), written by Jesse McLaren A 70-year-old with no cardiac history presented with 2 hours of chestpain radiating to the neck, associated with shortness of breath. Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. What do you think?
This case was texted to me by one of our residency graduates, and with the outcome, so I don't know how I would have interpreted it blindly. A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. is worrisome! 21, 2015 post by Dr.
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. He underwent PCI and had a good outcome. Ischemia comes and goes. mm of STE at 60 ms after the J-point in lead V3, 400 ms QTc, and 6 mm of R-wave amplitude in V4. Learning Points: 1.
These were texted to me only with "chestpain." It helps to know that the patient has active chestpain, as Wellen's is a post occlusion (reperfusion) state, with open artery and pain-free. Outcome: Patient ruled out for MI by troponins. And ECGs can change and evolve even when there is no ischemia.
Risk ratios (RRs) and mean differences with 95% CIs were computed for binary and continuous outcomes, respectively.RESULTS:Five randomized controlled trials with a total of 5727 patients were included, of whom 51.1% of patients had evidence of ischemia on a prior functional test. were referred to CCTA and 22.5%
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. Cardiology aware.
The Patient: A 57-year-old man who complains of a sudden onset of "sharp" chestpain while on a long bike ride. The pain does not radiate, and nothing makes it worse or better. ST depression in the setting of acute transmural ischemia (STEMI) is almost ALWAYS due to reciprocal change. He is pale, cool, and diaphoretic.
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS.
Brittany Weber, MD, PhD , of Brigham and Women’s Hospital, is the 2024 YIA winner for her abstract, "The Frequency, Prevalence, And Outcomes Of Incidentally Detected Coronary Artery Calcium Using Artificial Intelligence Analysis Among Patients With Immune Mediated Inflammatory Diseases.”
A 67 yo f developed chestpain this morning." There is probably a trickle of flow which is why there is both subendocardial ischemia (ST depression) and early subepicardial ischemia (hyperacute T-waves). Opiates are associated with worse outcomes in Myocardial Infarction. Am Heart J. 2005;149:1043–1049.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. For now she can only say Not OMI.
This is ischemia until proven otherwise. A fixed stenosis in that other artery, especially in the context of hypotension from the occlusion of the first coronary artery, can lead to ischemia and very poor LV function and worsening shock. I learned that the patient is on Sotalol for control of PVCs. This explains the long QT.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Finally, head-up CPR (which was not used here), makes for better resuscitation.
The patient with no prior cardiac history presented in the middle of the night with acute chestpain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. This is a case I had quite a while back. See the explainability : She sees large T-waves in V2, V3.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Ischemia may be so brief that Wellens' waves do not evolve 3. Lessons: 1.
There was no chestpain or SOB, at least none reported by Dr. Lee. Answer : There is very abnormal T-wave inversion in aVL which is typical of subtle transmural/subepicardial (due to occlusion) ischemia to the inferior wall. Given that this patient has no chestpain, one must be skeptical of such a diagnosis.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. His ECG is shown below. 118.007305) from Heitner et al. ,
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. Click here to sign up for Queen of Hearts Access Case 2: A woman in her 60s presented with acute chestpain. Outcome of case 2? Normal vital signs. Here is his ECG at triage: What do you think? Normal vitals.
Written by Pendell Meyers A woman in her 70s had acute chestpain and called EMS. The patient survived with unknown long term outcome. In this older woman with new chestpain — I find it difficult to justify not activating the cath lab. No further ECGs were recorded.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chestpain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. This is a case from many years ago that I discovered recently. He had been drinking 5 beers. No pericardial effusion.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Gottlieb SO, et al.
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. 2021 ACC/AHA ChestPain Guidelines.
A male in his 60's called 911 for chestpain. His pain was intermittent and he was vague about when it was present and when it was resolved. There is about 1 mm of STE in aVR I con sidered but rejected subendocardial ischemia. Is it subendocardial ischemia, or inferior MI? Here is his prehospital ECG: Diagnosis?
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center. 24 and find out what it all means for your patients.
The chestpain quickly subsided. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? Are you worried about OMI in this case?
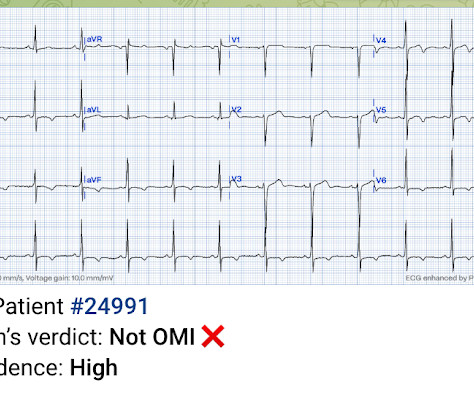
There is normal R-wave progression in the precordial leads with no evidence of ischemia. Just the fact of chestpain and highly elevated troponin is enough to activate the cath lab, but here you can see just how subtle hyperacute T-waves can be. Here the image quality is enhanced using the PM Cardio app. What do you think?
Now chestpain free. After midnight (now day 3), she complains of shoulder pain and dyspnea. Outcome and Analysis: ECG 1 is diagnostic of inferior and right ventricular MI. Furthermore, there are T-wave changes in V2 and V3 which are highly suggestive of ischemia, but difficult to localize: anterior?
She did not report any chestpain or pressure. She was brought to the Emergency Department and this ECG was recorded while she was still feeling nauseous but denied chestpain, shortness of breath, or other symptoms: What do you think? The morphology of STE is not diagnostic of being due to acute transmural ischemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content