This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
[link] A 30 year-old woman was brought to the ED with chestpain. It had started just after nursing her newborn, about an hour prior, and she described it as a severe non-pleuritic “pressure” radiating to the back. She had given birth a week ago, and she had similar chestpain during her labor.
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiac arrest. Ischemia comes and goes. The formula results in 23.43, just above the 23.4
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. Cardiology aware.
In the evening, a middle-aged man complained of chestpain at the nursing home. Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. His chestpain was vague. He mentioned "cancer" and "chest". He was awake, with a pulse of 130 and BP of 50/30. Fluids were started.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. V1 and aVR are often elevated in subendocardial ischemia.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. A 59 y/o Female calls 911 for crushing chest discomfort and difficulty breathing.
One of my most talented readers is a health care assistant (a nursing assistant) who has taken a keen interest in ECGs. Now chestpain free. Furthermore, there are T-wave changes in V2 and V3 which are highly suggestive of ischemia, but difficult to localize: anterior? And they teach me a lot. He can beat nearly anyone.
It’s an intubated septic nursing home patient." Acute chestpain and a bizarre ECG Bizarre (Hyperacute??) I thought the overall picture in these 6 chest leads did not look like acute OMI. I received this ECG in a text message, with the message: "Hey, these look like hyperacute T waves to me, what do you think?
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the Emergency Department with sudden onset chestpain that began 14-hours ago. The nurse alerted the MD because the patient was still symptomatic, diaphoretic and “looking unwell”. Shroff, G.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. All of the patients presented with chestpain , and they are all in triage. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia.
The patient was a 70-something yo previously healthy male on no medications who presented to the ED with epigastric pain, onset over a few hours. He denied chestpain of any sort and his vitals were all normal. They cannot be assumed due to LV strain ( and they cannot be assumed to represent ischemia ).
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. Lead V2 shows RR’ QRS configuration, and although ST depression is otherwise expected here, the discordance is a bit excessive.
A late middle-aged man presented with one hour of chestpain. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. It would be difficult to get a nurse to give it faster! Most recent echo showed EF of 60%.
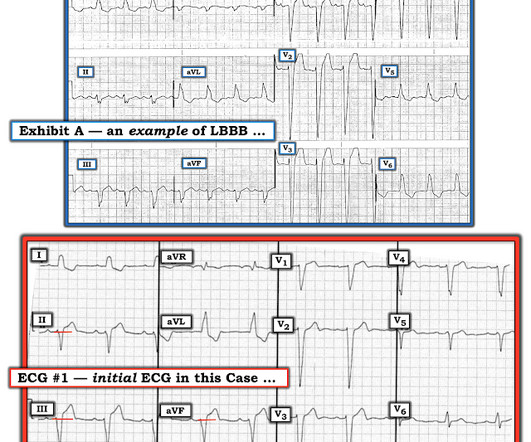
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content