This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
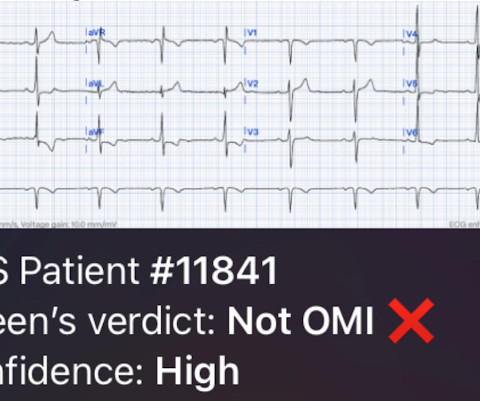
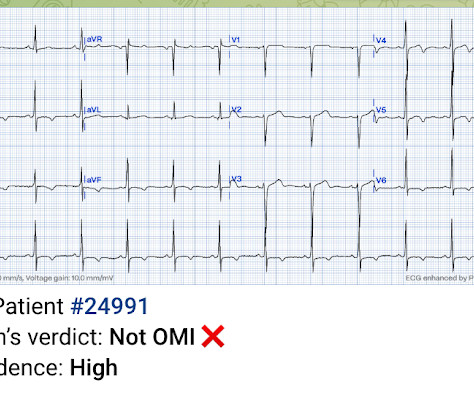
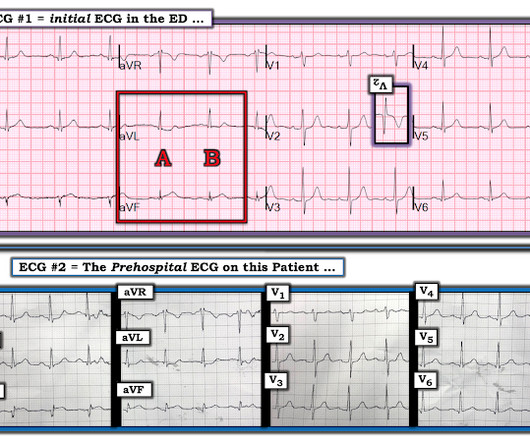
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
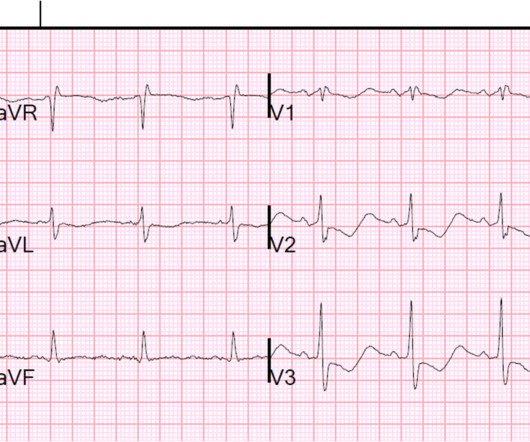
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. But are there any other signs of Occlusion MI? Curr Cardiol Red 2021 3. Kontos et al.
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. non-occlusive ischemia) Ongoing ischemic symptoms in NSTEMI is already an indication for emergent cath, regardless of the ECG.
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. STEP #2 = Clinical Impression — in which we correlate our assessment that we made in Step #1 to the clinical situation at hand.
Written by Jesse McLaren A 45 year old presented with two weeks of recurring non-exertional chestpain, now constant for an hour. Because of the ECG changes in a patient with chestpain, and with inferolateral hypokinesis on POCUS, the cath lab was activated. Below is old and then new ECG (old on top; new below).
Written by Jesse McLaren A 65 year old with a history of atrial flutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chestpain, which was ongoing at triage. The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. What do you think?
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. In this case, the EMS provider was routed to the urgent care facility.
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. It started while he was at rest after finishing a workout.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG? What is your next step?
A 41-year-old male who presents to the emergency department with chestpain. Patient reports approximately 2 hours prior to arrival he developed a sharp chestpain that radiates into his left arm and left lower leg. Describes the radiating pain as numbness/tingling. No shortness of breath. No recent travel.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6.
Written by Jesse McLaren Four patients presented with chestpain. Other signs of OMI that complement the ECG include new regional wall motion abnormalities and refractory ischemia References 1. This will make expert OMI interpretation widely available, and help us continue to learn the subtleties of ECG interpretation 4.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. He did not remember whether he had experienced any chestpain. He was intubated in the field and sedated upon arrival at the hospital. Here is his presenting ECG: ECG 1, t = 0 What do you think? He was admitted to cardiology.
Jesse McLaren discusses some key aspects of cocaine chestpain ECG interpretation in this month's blog including: Patients with cocaine-associated chestpain require benzodiazepines +/- nitroglycerine for symptom relief, aspirin and ECG to look for signs of occlusion and reperfusion.
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. The unique " shape " of the prominent ST-T wave abnormalities in this tracing — that are much more suggestive of some significant form of LVH ( L eft V entricular H ypertophy ) rather than ischemia. What do you think now?
Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. This confirms that the pain was ischemia and is now resovled. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Ischemia 3. The ST depression in precordial leads suggest still more widespread ischemia, so the exact culprit is not at all clear. He presented to the ED 1 day later: He stated that he had continued episodes of chestpain and then it became constant that morning (about 8 hours prior). Never assume chestpain is reflux.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Abstract 556.
A male in his 60's with no history of coronary disease presented with chestpain. I saw this ECG in a stack and noticed that caregivers had been only worried about ischemia. Here is his ED ECG: He had several previous ECGs this year and they were all identical. What do you notice? What should you do? VERY long QT).
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. Here is the history: A 40-something male had intermittent chest discomfort until 90 minutes prior to presentation, when it became constant. At 100 minutes, the above ECG was recorded.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The ECG was incorrectly interpreted as no signs of ischemia. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. His vitals were within normal limits.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chestpain with paresthesias of the left arm. A repeat ECG was recorded with pain 2/10: Not much change.
In a 57-year-old man with chestpain, an ECG obtained by EMS showed widespread ST-segment depressions. At the hospital, left main coronary-artery stenosis was seen on angiography (shown in a video).
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. As per Dr. Smith, in a patient with new chestpain — these flattened ST segments in leads V2,V3 suggest acute posterior OMI until proven otherwise. Here is his ED ECG: What do you think?
In EM Cases' first ECG Cases blog we review 7 examples of ECGs of patients presenting to the ED with chestpain, who's ECG were read as normal by the computer. And guess what.they all show acute ischemia!
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
A 20-something male drank heavily of ethanol and used cocaine, then was involved in a stressful verbal altercation, at which time he developed chestpain. 911 was called and the medics recorded this ECG (unfortunately, leads V4-V6 are missing) Due to marked ST Elevation, the computer read was STEMI What do you think?
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize. AI can do it too.
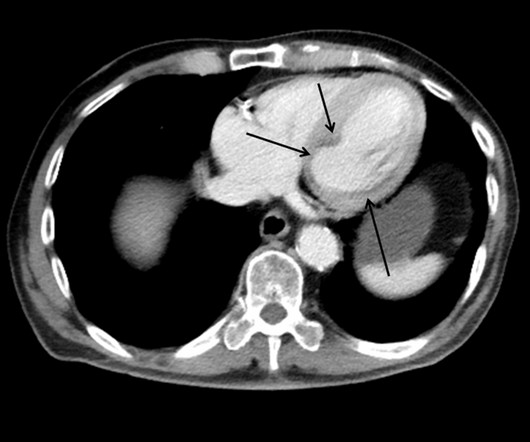
This case shows a CT image of subendocardial ischemia. This patient presented with a mechanical fall and had chestpain. His chestpain increased and this ECG was recorded: Now there is increasing inferior ST elevation. Severe Left Main disease, and chestpain with contrast injection into the LM.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This strongly suggests reperfusing RCA ischemia.
The patient presented with chestpain. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. Is this Acute Ischemia? More on LVH.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 2024, [link]. 22, 30 Nov.
The study describes the validation of Cleerly's artificial intelligence-guided quantitative coronary CT angiography (AI-QCT) ISCHEMIA technology for diagnostic accuracy and prognostic risk stratification. High Diagnostic Accuracy of AI-ISCHEMIA in Comparison to PET, FFR-CT, SPECT, and Invasive FFR: A Pacific Substudy. 2024.01.007.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content