This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Two subsequent troponins were down trending.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
He did not have chestpain. The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. Chestpain in high risk patient. Here is his triage ECG: What do you think? See these other relevant cases: What are these bizarre bigeminal PVCs?? Is it STEMI?
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
The patient was managed in the ICU and had serial troponins. At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4. It is worthwhile keeping in mind important findings from this study: More than 1/4 of all MIs are not accompanied by chestpain.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. E CG # 1 was obtained in the referral hospital, approximately 2 hours after the onset of chestpain. This ECG was recorded on arrival: What do you think?
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. Patients on dialysis often do not have chestpain in the setting of acute MI. Why is this?
Wellens' is a syndrome of a painless period following an anginal (chestpain) event. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. She also complained of generalized weakness, lightheadedness, diaphoresis, chestpain, and cough. What is the Diagnosis? She was discharged and did well.
He went into cardiogenic shock and is intubated in the cardiac ICU. I just got the follow up that he had a near complete very proximal LAD occlusion , and a complete PDA occlusion. Not the culprit artery I was expecting but potentially a wraparound LAD?
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it?
The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. A bed side echocardiography revealed a severely depressed LVEF of about 20-25%. When looking at the above ECG you will find that the QRS following ventricular pacing is very long.
And she does not know that this is an overdose; she thinks it is a patient with chestpain!! He was admitted to the ICU and was unstable, in shock, overnight. Case Continued: He was stabilized on more calcium, pressors, and high dose insulin. 3 hours later, this was recorded at a K of 2.8 mEq/L and total calcium of 14.7
Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8 Given the absence of chestpain — cardiac contusion is also unlikely. At that time his diastolic blood pressure was also hovering between 45 and 55 mmHg. There is no ECG available from this time.
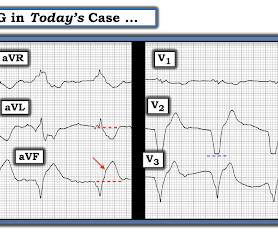
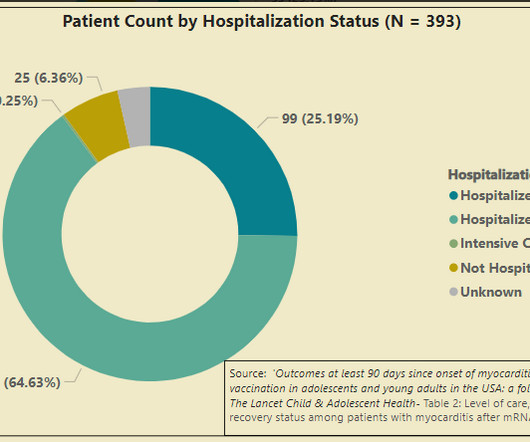
The current study should dispel the ludicrous notion that clinical myocarditis - a disease entity that comes to light when you have chestpain because cells in your heart are dying — is mild. The CDC study published in Lancet on previously healthy 12-29 years old’s is a survey-based study.
With OMI, all you know is that your patient has some nonspecific chestpain, SOB, shoulder pain etc. She was critically ill and required noninvasive positive pressure ventilation and ICU admission for suspected infectious respiratory illness. which is probably NOT due to acute MI.
A middle-age woman with no previous cardiac history called 911 for chestpain. As a result I got to witness first-hand how the incidence of primary VFib appeared to dramatically decrease in our ICU as a result of the new practice at that time of using prophylactic Lidocaine on acute MI patients.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content