This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. Due to the chestpain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. He had associated nausea, vomiting, and dyspnea.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Past medical history included diabetes and hypertension.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? A VSR is more likely to occur in patients who are older, female, hypertensive, have chronic kidney disease, and have no prior history of smoking.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history. Is it STEMI or NonSTEMI?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
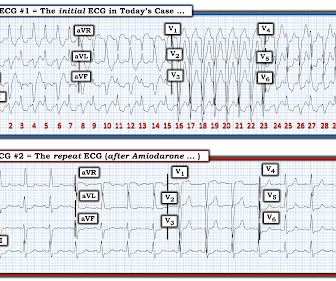
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. Chronic RVH is due to chronic pulmonary hypertension, and these patients are extremely difficult to manage when they are acutely ill. Lots of info here.
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
Written by Willy Frick with edits by Ken Grauer A woman in her 70s with a history of hypertension presented with acute onset shortness of breath. It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock).
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? He was intubated for altered mental status.
This 60-something with h/o COPD and HFrEF (EF 25%) presented with SOB and chestpain. Multifocal Atrial Tachycardia 2. P EARL # 4 — In “real life” — there is often NO distinct “cut-off” for differentiating between sinus tachycardia with multiple different-looking PACs vs MAT. Here is the ECG: What do you think?
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. There is some ST-segment elevation in DII, DIII, aVF, V4-6. What is the rhythm?
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? In addition to sinus tachycardia, the only abnormalities listed by the computer were "low voltage, precordial leads" and "anteroseptal infarct, old.Q Physician: "No STEMI."
No chestpain. In the context of today's case — these P waves are diagnostic of RAE = P Pulmonale ( See ECG Blog #75 ) and almost certain associated pulmonary hypertension. Retrospectively — I interpret this 1:1 retrograde conduction as diagnostic of a reentry SVT rhythm as the etiology of the initial tachycardia.
This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. Wellens' is a syndrome of a painless period following an anginal (chestpain) event. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. Tachycardia (or nearly) 2. Tachycardia, = 1.8. An ECG was texted to me (Smith) without any clinical information: What did I say?
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chestpain and shortness of breath off and on over the past three days, with associated vomiting. The rhythm is sinus tachycardia at ~105/minute. The rhythm is sinus tachycardia at ~115/minute.
The ECG in Figure-1 was obtained from an older woman — who presented with chestpain and palpitations over the previous hour. She had a history of hypertension, and was on medication for this — but she was otherwise healthy. BP = 140/90 mm Hg in association with the rhythm in Figure-1. Is this Ventricular Bigeminy?
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. A normal PR interval.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. Severe Tachycardia Acute Coronary Syndrome (obstructive coronary disease) a. This results in Type I MI.
Palpitations in a Young Healthy Male A pathognomonic ECG you should recognize instantly A middle-aged man with severe syncope, diffuse weakness Chestpain and Diffuse ST depression, with STE in aVR. Does this patient have hypertension and/or heart failure that has worsened? You probably think it is left main.
This results in severe chestpain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. Hypertension and diabetes were the two most common risk factors identified. It can cause diminished heart function and mortality if not treated properly with suitable measures.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. This was contributed by some folks at Wake Forest: Jason Stopyra, Shannon Mumma, Sean O'Rourke, and Brian Hiestand.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The syncope lasted about 2-3 minutes according to his wife.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis? Now another, with ultrasound.
ACS QID 3103 A 64 year old Caucasian male with a history of extensive tobacco use, hypertension, hyperlipidemia, and obesity presents with acute onset chestpain. His exam was notable for tachycardia, elevated jugular venous pressure, diffuse rales, and an early 2/6 systolic murmur loudest at the cardiac apex. Question 2.
A late middle-aged man presented with one hour of chestpain. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. In multivariate analysis, serum potassium level was negatively and age positively related to ventricular tachycardia. Most recent echo showed EF of 60%.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. Ventricular tachycardia?) Improved chestpain is unresolved chestpain.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. History Patient complains of a 24-hours of chestpain of sudden onset, sharp in nature. Denies SOB.
Written by Magnus Nossen The below ECG was obtained from a 65 year old man with ongoing chestpain. He has a history of hypertension an d tobacco use. The below ECG was obtained 45 minutes after the first one with the patient being free of chestpain at the time of recording of ECG #2. He is otherwise healthy.
He denied chestpain. A Chest X-ray did not show pulmonary edema. This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. It is correct that he did not have chestpain, but we must remember that fully 1/3 of full blown STEMI do not present with chestpain.
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. A 30-something woman with chestpain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chestpain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation.
Written by Hans Helseth, with edits and comments by Smith and Grauer An 84 year old man with chronic hypertension and CKD presented to a primary care clinic. He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. Does this patient have ACS Symptoms?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content