This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The culprit was opened and stented.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had no chestpain. The hypertension alone is the likely etiology of the pulmonary edema. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. He had a history of hypertension, but no history of heart problems. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? Note the beginning of Wellens' (reperfusion T-waves) in V3-V6.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. She is somewhat hypertensive, but her vital signs are otherwise normal. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history. Is it STEMI or NonSTEMI?
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chestpain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
He learned more about the patient: A 77 year old female with a past medical history of hypertension and hyperlipidemia presented to the ED at around 0520 after waking up at 0400 with 10/10 chest heaviness radiating to both arms. The patient had continued to have chestpain. The cath lab was activated.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. <0.049 ng/mL).
Clinical introduction The patient was a man in his 40s with a medical history of hypertension, Behcet’s disease (BD) and chronic renal dysfunction. He was admitted to our hospital with issues of chestpain, shortness of breath and heart palpitations without any obvious inducement.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
Case submitted and written by Dr. Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain.
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. There is sinus rhythm with PACs and PVCs.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. Fortunately, that is exactly what happened.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss.
This is by Magnus Nossen, from Norway The patient is a 70 something male with a hx of hypertension and tobacco use disorder. The patient contacted EMS after a few hours of chestpain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder. The culprit lesion was opened and stented.
What do you think of this ECG in a patient with chestpain? Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chestpain. The pain had been mild and intermittent for 2 weeks, but had become more intense on the night of presentation. Is the ST elevation due to LVH?
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. A mid-LAD culprit lesion was identified and stented. Below are two examples of this.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. Here is the angiogram after stent placement.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Two stents were placed with resultant TIMI 3 flow.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. You must record frequent serial ECGs for patients with chestpain.
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. Patients on dialysis often do not have chestpain in the setting of acute MI. Why is this?
While men often report crushing chestpain as the most prominent symptom, women might experience subtler symptoms like shortness of breath, nausea, or back pain. Women might describe it as a tightness, pressure, or squeezing sensation rather than a sharp pain.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Women also had more cardiovascular risk factors, including hypertension (66.6%
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow.
A late middle-aged man presented with one hour of chestpain. This was stented. He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Most recent echo showed EF of 60%. He had recently had a NonSTEMI.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? He did well.
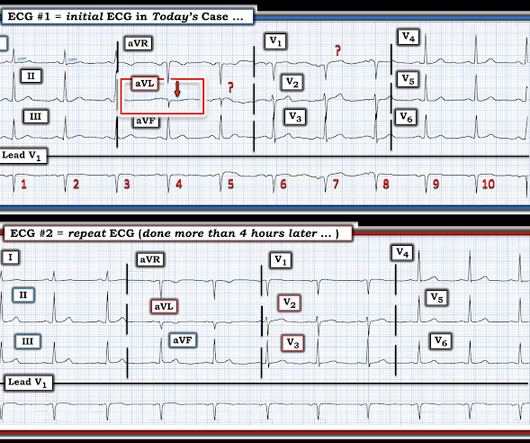
Written by Magnus Nossen The below ECG was obtained from a 65 year old man with ongoing chestpain. He has a history of hypertension an d tobacco use. The below ECG was obtained 45 minutes after the first one with the patient being free of chestpain at the time of recording of ECG #2. He is otherwise healthy.
Written by Magnus Nossen The ECG below was obtained from 50-something male with a history of hypertension and tobacco use. The patient contacted the ambulance service after he experienced sudden onset chestpain and diaphoresis that had started 20 minutes prior. The above ECG is from man in his 80s with crushing chestpain.
Written by Willy Frick A man in his 60s with hypertension and prior stroke presented with three days of crushing chestpain. He reported intermittent chestpain for the last few months, but never lasting this long. The cardiology consultant notes that pain is "almost resolved." There is active infarction.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. After stent placement: The vessel is now open with TIMI 3 flow, although it is diffusely diseased and the middle segment is ectatic.
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. It was treated with a drug eluting stent. It is awaiting FDA approval (but approved for 1.5 The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent").
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He carries the diagnoses hyperlipidemia, hypertension, and diabetes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content