This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. Due to the chestpain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. He had associated nausea, vomiting, and dyspnea.
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity.
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. It started while he was at rest after finishing a workout.
This results in severe chestpain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. Hypertension and diabetes were the two most common risk factors identified. It can cause diminished heart function and mortality if not treated properly with suitable measures.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think?
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
High blood pressure, also known as hypertension, is a common condition that affects millions of people worldwide. Often referred to as the silent killer, hypertension can quietly damage your heart and other vital organs over time. Hypertension is diagnosed when blood pressure consistently reads 130/80 mm Hg or higher.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Past medical history included diabetes and hypertension.
A 60-something male presented stating that he had had chestpain that morning which awoke him from sleep but then resolved after several minutes. He has had similar pain in the past which he attributed to acid reflux. He has a history of untreated hypertension. He is pain free now. His systolic BP was 200.
He stated that it is "an acute change from previous" in an elderly smoker with hypertension, syncope, and abdominal pain. 33 yo male with 2 days of chestpain This was an anterior STEMI that had apical ballooning and was wrongly thought to be Takotsubo Diffuse ST Elevation with Apical Ballooning: is it Takotsubo Stress Cardiomyopathy?
He had had several episodes of pain since onset; it was described as pressure-like and lasts about 5-15 minutes and resolves spontaneously. He had been pain free for about an hour. He had some "pre-diabetes ," but no h/o hypertension, no known family history of heart disease, and he smokes about 1-2 cigarettes per day.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. He had a history of hypertension, but no history of heart problems. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think?
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. She is somewhat hypertensive, but her vital signs are otherwise normal. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history. Is it STEMI or NonSTEMI?
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chestpain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. What About Lead V4?
He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder. The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
The National Institute for Health and Care Excellence (NICE) advise against routine testing for coronary artery disease (CAD) in patients with non-anginal chestpain (NACP). Patients in group 3 were more likely to be hypertensive (p=0.008) and have higher Qrisk2 scores (p<0.001) when compared with those in group 1.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. Chronic RVH is due to chronic pulmonary hypertension, and these patients are extremely difficult to manage when they are acutely ill. Lots of info here.
An 80-something woman who presented with chestpain and dyspnea. An old formal echo was found from 6 mo ago: Dilated right ventricle with septal flattening and estimated right ventricular systolic pressure of 70 mmHg (significant pulmonary hypertension). After all, this patient did also present with chestpain. ) — See below.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. What do you think? This ECG is more difficult.
Non-ischemic phenotypes differed in the prevalence of hypertensive response, reduced CR, and reduced HRR. ConclusionsFour non-ischemic phenotypes of low-risk NSTE-ACS patients were identified: near-normal type, inotropic insufficiency type, hypertensive type, and chronotropic insufficiency type.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Interestingly, this patient was seen in the ED for hypertension and headache 3 days earlier. Sent by Pete McKenna M.D.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. <0.049 ng/mL).
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
A 63-year-old woman presents to the office for a second opinion on chronic chestpain and heart failure management. She has a medical history of mixed connective tissue disease, obstructive sleep apnea, hepatic steatosis, and long-standing hypertension diagnosed in her twenties.
A VSR is more likely to occur in patients who are older, female, hypertensive, have chronic kidney disease, and have no prior history of smoking. Not all patients with acute ( or recent ) MI have chestpain with their event. I thought the presentation of today's case makes it worthwhile to review the data regarding this issue.
Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Evaluation of these pts results in substantial costs for unnecessary hospitalization and extensive testing. Length of stay (LOS) in the CPU to discharge was 10.4
A 30-something woman with chestpain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chestpain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
He learned more about the patient: A 77 year old female with a past medical history of hypertension and hyperlipidemia presented to the ED at around 0520 after waking up at 0400 with 10/10 chest heaviness radiating to both arms. The patient had continued to have chestpain.
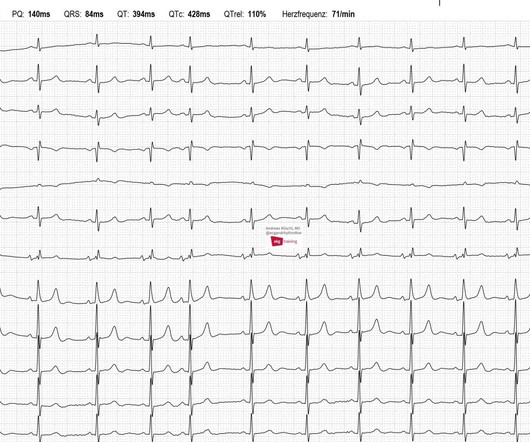
This is the ECG of an 81-year-old man with hypertension. Currently, he has no complaints: no palpitations, no shortness of breath, no syncope, no chestpain. The rhythm is irregular, but all P-waves have the same shape. There are no consequences for the patient resulting from this diagnosis.
This is the ECG of an 81-year-old man with hypertension. Currently, he has no complaints: no palpitations, no shortness of breath, no syncope, no chestpain. The rhythm is irregular, but all P-waves have the same shape. There are no consequences for the patient resulting from this diagnosis.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. See this case: A man his 50s with chestpain.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content