This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This results in severe chestpain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. The average hospital stay was 8.51 (SD7.2) days while In-hospital mortality was 8.8%. were male, with the average age of 56.313.5
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. The sinus tachycardia is a definite concern that something acute may be ongoing. The patient arrested outside the hospital.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chestpain. Upon EMS arrival the patient appeared acutely ill and complained of chestpain. An ECG was recorded immediately and is shown below.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. The patient had a protracted hospitalization and did not survive.
Let me tell you about her hospitalization, discharged 1 day prior, but it was at another hospital (I wish I had the ECG from that hospitalization): The patient is 40 years old and presented to another hospital with chestpain and SOB. Probably because of a high troponin with chestpain.
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. The ECGs show a wide complex, irregularly irregular tachycardia. At this point, the patient had been symptomatic for almost 5 hours, appeared unwell with chestpain and diaphoresis.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. Admitted to the hospital service for further evaluation and management." The Importance of the History: As noted above — the onset of chestpain in today's case was acute.
She presented to an outside hospital after several days of malaise and feeling unwell. Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? At the time of admission, her vital signs were normal.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history. Is it STEMI or NonSTEMI?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Just as important is pretest probability: did the patient report chestpain prior to collapse? For clarity in Figure-1 — I've reproduced today's ECG — obtained following successful resuscitation of out-of-hospital cardiac arrest. After cardiac arrest, I ALWAYS wait 15 minutes after an ECG like this and record another.
Dr Sanjay Gupta, a consultant cardiologist at York Hospital, is an expert in POTS, or postural tachycardia syndrome. The post York Hospital Consultant Could Have Treatment to Tackle Long Covid appeared first on Dr Sanjay Gupta Cardiologist. The symptoms can last for years, ruining patients’ lives. Read more here.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
A man in his 40's with a h/o coronary disease complained of sudden dizziness and chestpain. Alternatively, it could be posterior fascicular ventricular tachycardia. Either the PSVT was broken and restarted, or there is sinus tachycardia. Outcome: The etiology of the patient's sinus tachycardia was not discovered.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The proximal LAD is now widely patent.
He was treated for infection and DKA and admission to hospital was planned. While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest.
Finally, the presentation is dyspnea, not chestpain. This was what was found: She had been at a different hospital less than a week ago at which time she had an an RCA stent for an lesion that had TIMI-3 flow. Patients with anterior LV aneurysm usually have poor LV function and heart failure. What is the Lesson to be learned?
He did not have chestpain. ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Chestpain in high risk patient. Here is his triage ECG: What do you think? Is it STEMI?
A few days into her hospital stay she developed chest discomfort and the following ECG was recorded. The ECG below was on file and was taken a few days earlier, on the day of admission to the hospital. The chestpain quickly subsided. She is healthy with no known cardiac disease. What do you think?
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? He was intubated for altered mental status.
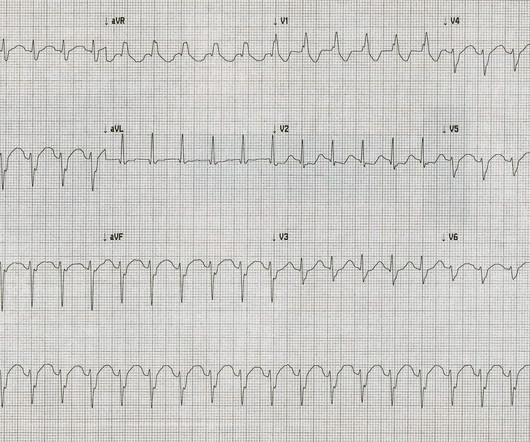
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute. Figure-2: I've labeled the initial ECG. The QRS complex is obviously wide.
His confusion progressively dissipated enroute to the hospital. There was no chestpain. At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The fall was not a mechanical etiology. The ED activated trauma services, and a 12 Lead ECG was captured. Type II ischemia.
The ECG in Figure-1 was obtained from a 90-year old woman — who presented with a 2-to-3 day history of chestpain, that became worse on the day of admission. That said — the important point is her ongoing ( and increasing ) chestpain. C ASE F ollow- U p: The patient's chestpain was controlled.
The patient was promptly admitted to the hospital for further evaluation. Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. An initial electrocardiogram (ECG) is provided below. What do you think? What is the rhythm?
Written by Willy Frick A 57 year old man with was admitted to the hospital with chestpain. The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 1 remained in the hospital overnight.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
Postablation chestpain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02) years, colchicine did not reduce a composite of emergency department visit, cardiovascular hospitalization, cardioversion, or repeat ablation (29 versus 25 per 100 patient-years; HR, 1.18 [95% CI, 0.69–1.99];P=0.55).CONCLUSIONS:Colchicine
Apparently he denied chestpain. Other than tachycardia, Other than slight tachycardia, vitals were within normal limits (including oxygen saturation). JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. Here is his first ED ECG: What do you see?
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. He was prescribed apixaban.
There is sinus tachycardia (do not be fooled into thinking this is VT or another wide complex tachycardia!) What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. in-hospital mortality was 18.8% Protocols can be overridden by Physician Judgment.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Reverted to atrial fibrillation with RVR while in the hospital 3 times and needed cardioversion. Sinus tachycardia does not go this fast.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The patient was extubated on Day-3 of the hospital stay. The below ECG was recorded.
After admission to the hospital, the patient was discharged from the hospital without any investigation of his acute MI. In such cases, it is common for tachycardia to exaggerate the ST Elevation And, in fact, there was no new acute MI at this visit - troponins did not rise again. Many MI do not have chestpain 4.
MY Thoughts on ECG #1: The rhythm is sinus tachycardia at 105-110/minute. LEARNING Point: Maximal ST depression in leads V2-thru-V4 ( especially when the ST-T waves are shaped as they are in ECG #1 ) in a patient with new chestpain ( or sudden cardiac arrest, as in today’s case ) — is diagnostic of acute Posterior OMI until proven otherwise!
PEARL # 2: The way in which I look for flutter waves is to carefully set my calipers at precisely HALF the R-R interval o f the tachycardia ( since IF the rhythm is AFlutter — then the atrial rate should be twice the ventricular rate if there is 2:1 AV conduction ). She was discharged from the hospital on Amiodarone. See text ).
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Now the patient is in sinus tachycardia. Sinus tachycardia, AFlutter and ATach do not do this.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it?
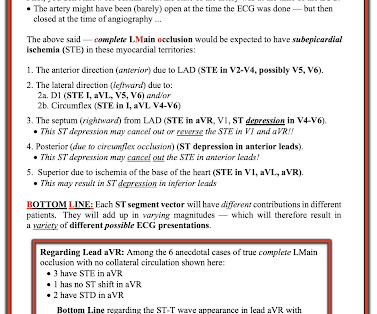
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. However, STE-aVR with multilead ST depression was associated with 31% in-hospital mortality compared with only 6.2%
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content