This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. The patient survived the hospitalization.
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
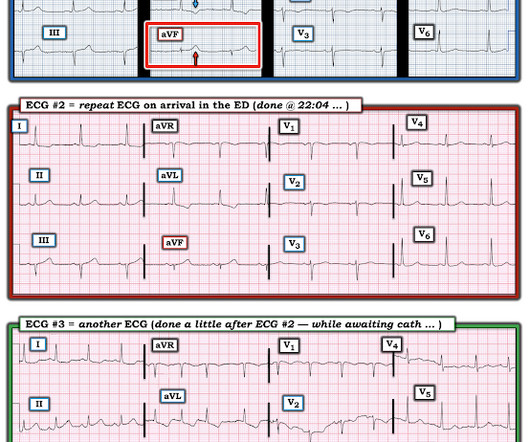
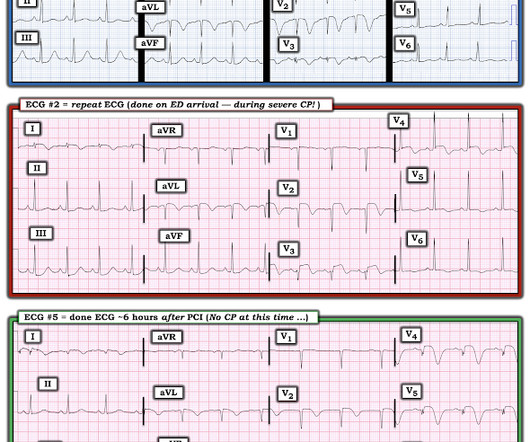
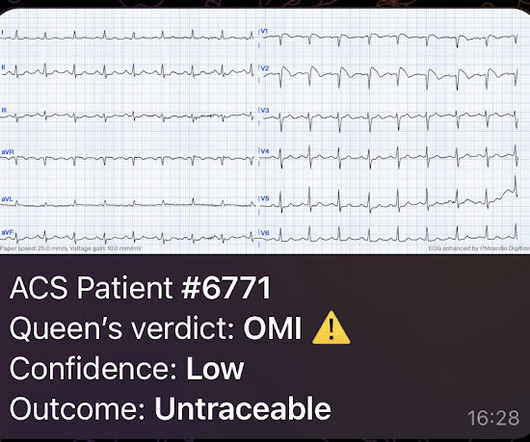
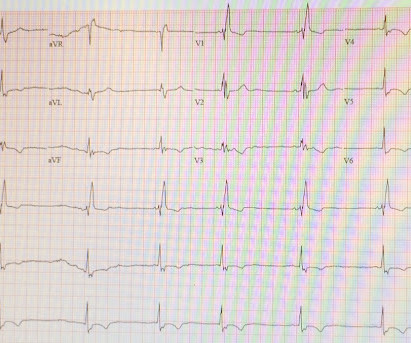
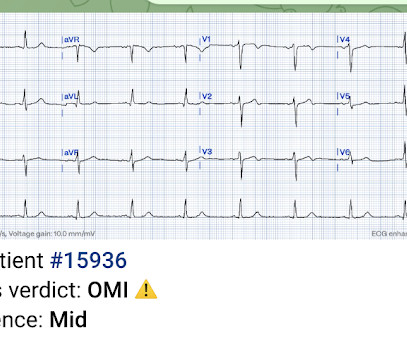
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability.
He was intubated in the field and sedated upon arrival at the hospital. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. When EMS arrived the patient was in ventricular fibrillation.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
I was working at triage when the medics brought this patient who is 65 yo and has had chestpain for 12 hours. It was opened and stented. This was a weekend late evening, and so it took time the cath team to get in to the hospital. They recorded a prehospital ECG at 2112 and said that it was “normal”.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. Admitted to the hospital service for further evaluation and management." The Importance of the History: As noted above — the onset of chestpain in today's case was acute.
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
A 55 years old diabetic male patient who had 12 stents in his heart underwent a successful beating heart bypass surgery under Dr. Prateek Bhatnagar, Director Cardiac Surgery. The patient was suffering with angina (chestpain) since 2002. The last 3 stents were placed just 6 months back but were not working.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc. This was written by Sam Ghali ( @ EM_RESUS ), with a few edits by me.
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history. This includes: 1.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. Also, we know the patient had a stent. Finally, the presentation is dyspnea, not chestpain. A few days before that, she had had an LAD stent for LAD occlusion. I was texted this ECG just as I was getting into bed.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). Amazingly, he did not suffer any serious complication in hospital.
This patient had the onset of chestpain 24 hours before arrival to the ED. An ECG was recorded immediately at triage and, at this hospital, the Queen of Hearts is routinely used to determine cath lab activation. The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
As discussed in many posts in this ECG Blog — despite not satisfying the millimeter-based definition of a STEMI — in this patient with new chestpain, the ECG findings in Figure-1 merit prompt cath lab activation without any need to wait for serum troponin to return elevated ( See ECG Blog #193 — regarding the new "OMI" paradigm ).
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. The following are the KEY clinical and ECG features that establish the diagnosis of W ellens ' S yndrome : There should be a history of prior chestpain that has resolved at the time the defining ECG is obtained.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. He had been seen several weeks ago at an outside hospital for a similar issue and had been discharged home, presumably after unremarkable workup.
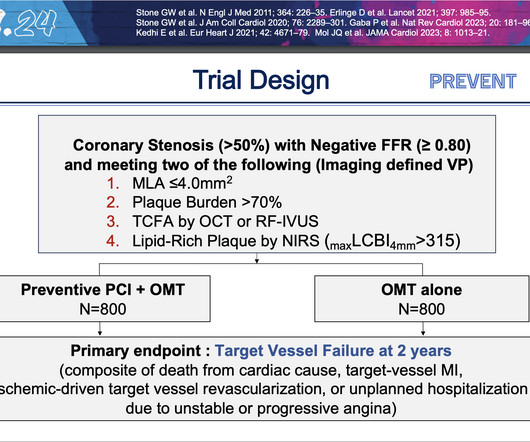
At two years, people who underwent preventive PCI were 89% less likely to experience the composite primary endpoint of cardiac death, heart attack in the target vessel, revascularization due to ischemia in the target vessel or hospitalization for unstable or progressive chestpain compared with people who received medications alone.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The proximal LAD is now widely patent.
I immediately looked for old charts, which were only available from another hospital, and an old echo confirmed inferior "akinesis" (which may also have persistent ST elevation). The patient's chestpain had resolved by the time of the ECG 2. Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
He was treated for infection and DKA and admission to hospital was planned. While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest.
While in the hospital, he had witnessed ventricular fibrillation (VF) arrest for which he received external defibrillation. He had minimal in-stent restenosis on angiography but had only minimal cardiac enzyme elevation and did not have antecedent chestpain before either of his events.
Ella Dunmore, who is a mother and former soldier, made the decision to seek medical attention, she had been experiencing headaches, chestpain, and shortness of breath for several weeks. John Hospital in Detroit and director of mechanical circulatory support. Ella went back to her house the following day.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. Patient 1 remained in the hospital overnight.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. So the RCA was stented.
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. You must record frequent serial ECGs for patients with chestpain.
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." Chestpain or discomfort) What do you think? The total duration of chestpain was 30-45 minutes.
She was admitted to the hospital with clinical signs of infection. Decision was made to stent the lesion. ECG#4 (below) was recorded about one year after the hospital stay described above. * During ECG #1 patient was febrile with a temperature of 40 °C, (104 °F) * Maximum Troponin I was 4210ng/L. What do you think?
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. There is sinus rhythm with PACs and PVCs.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chestpain associated with shortness of breath for the last 2 days. This was her ECG (it is unclear if this was with or without pain): Computerized ECG Read: “Normal sinus rhythm. This case was written by Sam Ghali: ( @EM_RESUS ). Normal ECG.”
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow.
No patient with chestpain should be sent home without troponin testing. All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. The patient was sent home with a prescription for omeprazole to treat presumed peptic disease.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. It is a matter of time." Do you want to see it? It is not subtle any more.
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)?
Troponin profile The patient underwent angiography and had a 90% thrombotic proximal LAD lesion that was stented. I focus my attention on the first 2 ECGs, both of which were done prior to arrival in the hospital. The patient is a 40-something year old man with new chestpain.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. He arrived to our hospital one hour later. STE in lead I and II are more subtle. A second ECG was taken at 15:16.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content