This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. The patient arrested outside the hospital. KEY Points: Use of this systematic 2-Step approach does not slow you down.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. This is OMI until proven otherwise.
Hospital evaluation for this patient was negative for an acute coronary syndrome ( ie, CT coronary angiogram was normal — troponin was not elevated — and Echo was negative, with no sign of pericardial effusion ). The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen.
It is not always possible to be certain about the origin of chestpain just by its characteristics as the variation between individuals is quite a bit. A medical opinion should be sought in case of any significant chestpain so that important ailment is not missed. A pain lasting more than 30 minutes is usual.
She presented to an outside hospital after several days of malaise and feeling unwell. This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Electrocardiographic diagnosis of postinfarction regional pericarditis Oliva PB.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
This is a previously healthy male teenager who was awoken by chestpain. He was seen at another hospital and found to have a slightly elevated troponin, then underwent a CT pulmonary angiogram (PE) protocol which revealed a right sided pneumonia. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
Pericarditis refers to inflammation of the pericardium The pericardium is a sac within which the heart sits. Acute inflammation of this sac is known as acute pericarditis. About 5% of patients who present to A+E with chestpain which is not deemed to be a heart attack or angina are ultimately diagnosed with pericarditis.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). Amazingly, he did not suffer any serious complication in hospital.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She felt nauseous and lightheaded with no neurologic deficits.
3 hours prior to calling 911 he developed typical chestpain. This rules out pericarditis, which essentially never has reciprocal ST depression. This is not pericarditis because: a. Pain was typical for MI (substernal, not postional or sharp, resolved with NTG) b. Pericarditis does not have reciprocal depression.
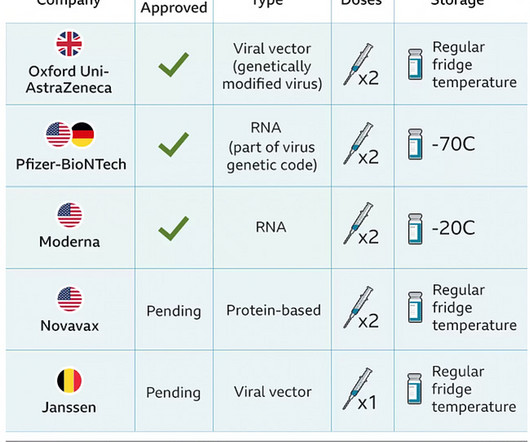
The case reports Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain.
In fact, there was no chestpain either. Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation.
Postablation chestpain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02) Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) 2.02];P=0.89). 11.53];P<0.001). 1.99];P=0.55).CONCLUSIONS:Colchicine
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. There is sinus rhythm with PACs and PVCs.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Massive Transfusion for Motorcycle Collision with Hemorrhage, Troponin Elevated. ST depression. Myocardial Contusion?
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. Such an out-of-proportion STE is virtually never seen in pericarditis. He arrived to our hospital one hour later.
Apparently he denied chestpain. As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain.
You do NOT see this in normal variant STE, nor in pericarditis. After admission to the hospital, the patient was discharged from the hospital without any investigation of his acute MI. At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. He was prescribed apixaban.
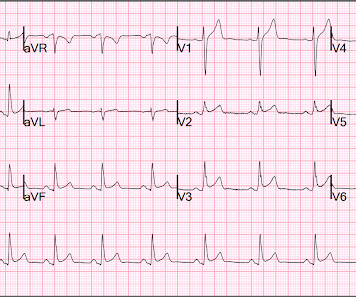
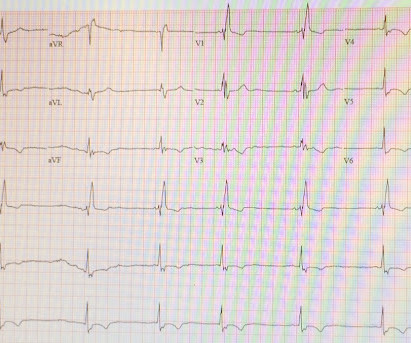
No chestpain. In a previously healthy adolescent ( who is 15 years old in today's case ) — the presentation of an acute febrile illness that is without a complaint of chestpain, is highly unlikely to be due to an acute MI. He was hemodynamically stable. How would YOU interpret the ECG in Figure-1 ?
Additionally, the App also includes a chestpain section, namely EDACS risk score, which is already a well known and validated tool for the approach to acute chestpain (many thanks for its developers and their courtesy for letting us to use it in our App, Martin Than, MD; John Pickering, BSc, PhD, BA and Dylan Flaws, MSc, PhD).
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Post-infarction Regional Pericarditis (PIRP) PIRP happens when MI is transmural, all the way from subendocardium to subepicardium, thus leading to inflammation of the subepicardium (next to the pericardium).
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? She was discharged after a short hospitalization with oncology and cardiology follow-up. The second most common cause of medical cardiac tamponade is acute idiopathic pericarditis.
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. The vast majority of cases of vaccine myocarditis requires hospitalization for monitoring for deterioration. He subsequently describes having sharp chestpain over the next few weeks.
Written by Kirsten Morrissey, MD with edits by Bracey, Grauer, Meyers, and Smith An older teen was transferred from an outside hospital with elevated serum troponin and and ECG demonstrating ST elevations. The workup at the transferring hospital yielded elevated troponin I at 18.1 He reported 1.5 mg/L and a normal WBC of 8.8.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content