This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
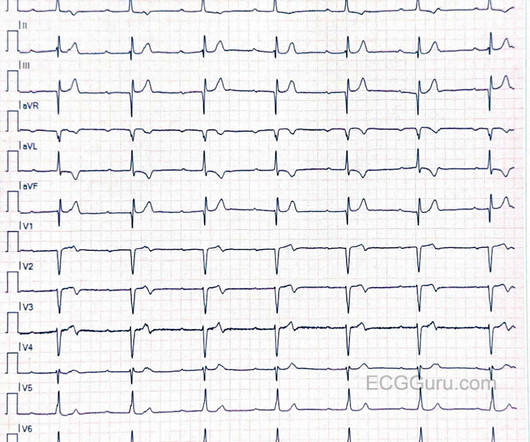
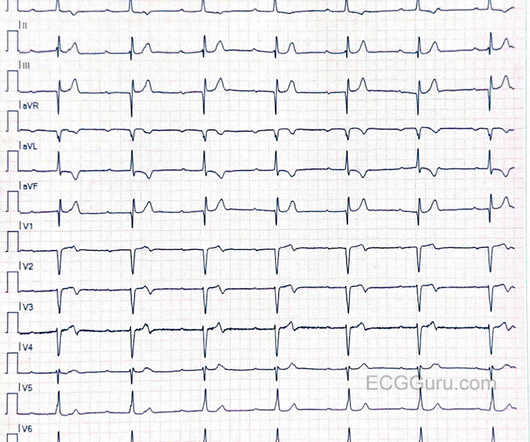
I do not know if this patient has a history of cardiac disease or a recent complaint of chestpain, but T wave inversion and some biphasic T waves makes me think of reperfusion changes, reflecting a recent M.I. We do not have followup on this patient's hospital course or treatment. 1) Is this rhythm the result of OMI?
I do not know if this patient has a history of cardiac disease or a recent complaint of chestpain, but T wave inversion and some biphasic T waves makes me think of reperfusion changes, reflecting a recent M.I. We do not have followup on this patient's hospital course or treatment. 1) Is this rhythm the result of OMI?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
An 80-year-old man with renal disease on hemodialysis, coronary artery disease, complete heart block and a dual chamber leadless pacemaker (LP) implanted because of previous bacteremia, presented with syncope. While in the hospital, he had witnessed ventricular fibrillation (VF) arrest for which he received external defibrillation.
This case was sent by Dr Avinash Krishnamurthy, a fine emergency medicine resident from Australia Cairns base hospital Case : An adolescent male had a mechanical fall and injured his left shoulder and arm. There was apparently no syncope and he had no bony injuries, but he did complain of left sided chestpain. Is there STEMI?
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Pain was severe and persistent. CT angiography chest assessing for PE and dissection negative. Heparin drip was initiated. Is there STEMI?
He presented with chestpain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. He presented with chestpain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Learning points *A patient with tachydysrhythmia and chest discomfort needs immediate rhythm or rate control. small squares in width (260ms).
Patients use them to observe their heart activity by themselves when they are not in the hospital. Though their accuracy is not as high as a hospital ECG machine, they are very beneficial in detecting problems in any medical emergency and providing information about long-term heart activity.
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. Given this patient's older age — if nothing "fixable" is found, she most likely has SSS ( S ick S inus S yndrome ) and will need a pacemaker ( See ECG Blog #342 for more on SSS ).
The patient was promptly admitted to the hospital for further evaluation. Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. An initial electrocardiogram (ECG) is provided below. What do you think? What is the rhythm?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The patient was extubated on Day-3 of the hospital stay. The below ECG was recorded.
Case An elderly patient had acute chestpain and 911 was called. The medics recorded the following initial ECG at time 0: The computer read (see below) gives no further comment beyond ventricular pacemaker. About 10 minutes later, and shortly before arrival at hospital (NOT Hennepin!), What do you think?
Hospital transport was unremarkable. He received a permanent pacemaker during the subsequent inpatient stay. Smith and Myers found that in otherwise classic Wellens syndrome – that is, prior anginal chestpain that resolves with subsequent dynamic T wave inversions on the ECG – even the T waves of LBBB behave similarly. [2]
See these similar cases: A man in his sixties with chestpain Why is there inferior ST elevation, and would you get posterior leads? Because of its potential for invoking uneeded cardiac catheterization or hospital admission — it is worth periodically reviewing this ECG pattern. Is it inferior and RV OMI?
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Syncope with Exertion (EGSYS) 7.
When a person experiences a heart attack or myocardial infarction, they may feel chestpain and other symptoms in different parts of their body. The Golden Hour post the Myocardial infarction (MI) It is a matter of great concern that 50% of individuals experiencing an acute heart attack pass away before reaching the hospital.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content