This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
IntroductionAcute coronary syndrome refers to a group of diseases characterized by sudden, decreased blood supply to the heart muscle that results in cell death, also known as acute myocardialinfarction. The majority of patients (67.9%) have been diagnosed with ST- Elevated MyocardialInfarction and were classified as Killip class I.
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. The patient survived the hospitalization. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. Peak troponin was not recorded.
This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
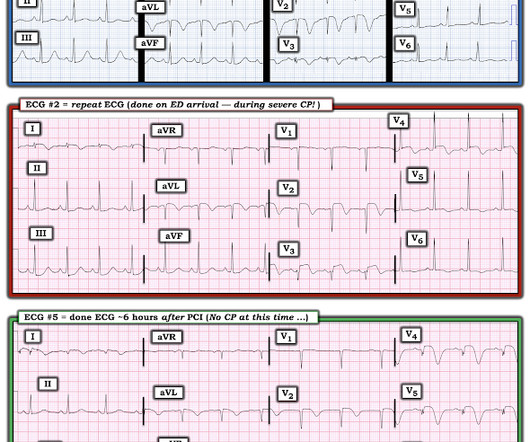
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. In any case, it is diagnostic of OMI in a chestpain patient. The family filed a lawsuit against the physician and the hospital.
Background Patients who experience acute myocardialinfarction (AMI) are at risk of recurrent AMI. Contemporary data on recurrent AMI and its association with return emergency department (ED) visits for chestpain are needed. Return ED visits for chestpain occurred in 27.0% (2017/7467) of index AMI survivors.
BackgroundRecent evidence highlights an increasing incidence of myocardialinfarction in young women. years]) admitted to the China ChestPain Center Database between 2016 and 2021. years]) admitted to the China ChestPain Center Database between 2016 and 2021.
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
She presented to an outside hospital after several days of malaise and feeling unwell. This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). At the time of admission, her vital signs were normal.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. Acute myocardial injury: Is it myocardialinfarction, or perhaps myocarditis?
Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. But because the patient had no chestpain or shortness of breath, it was not deemed to be from ACS. Clinical characteristics of dialysis patients with acute myocardialinfarction in the United States.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
BackgroundThe circadian rhythm of myocardialinfarction (MI) in patients with obstructive sleep apnea (OSA) remains disputable and no studies have directly evaluated the relationship between nocturnal hypoxemia and the circadian rhythm of MI. Journal of the American Heart Association, Ahead of Print.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
Resource use consumption data were collected from all study participants and hospital cost data from US participants (n=1125) to estimate total medical costs. The primary and secondary economic outcomes were total costs at 12 months and at 45 days, respectively, from the US health care system perspective.
He was treated for infection and DKA and admission to hospital was planned. While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. He had been seen several weeks ago at an outside hospital for a similar issue and had been discharged home, presumably after unremarkable workup.
He has now implemented the Queen of Hearts in his hospital. A 55 year old with no previous cardiac history presented with 3 hours of chestpain. The pain was persistent and reportedly still present at the time of the ECG. Translation from French: Acute Occlusion MyocardialInfarction with High Confidence.
Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Evaluation of these pts results in substantial costs for unnecessary hospitalization and extensive testing. Length of stay (LOS) in the CPU to discharge was 10.4
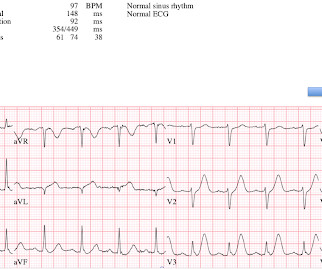
He had no medical history of myocardialinfarction (MI). He was admitted to our hospital with issues of chestpain, shortness of breath and heart palpitations without any obvious inducement. A 12-lead ECG indicated sinus rhythm with a heart rate of 78 bpm.
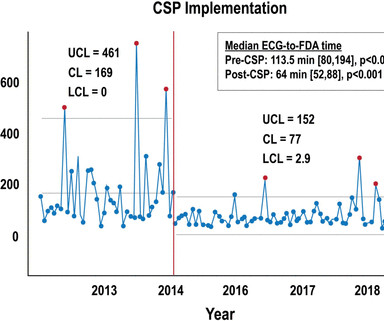
Background Patients who experience in-hospital ST-segment elevation myocardialinfarction (iSTEMI) represent a uniquely high-risk cohort owing to delays in diagnosis, prolonged time to reperfusion and increased mortality. Statistically insignificant numerical reductions were observed post-CSP in in-hospital mortality (18.2%
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chestpain who was headed to an outside hospital (which happens to be a catheterization center).
More than 8 million Americans visit hospital emergency departments experiencing chestpain every year. “In the future, patients with coronary inflammation can be identified by the CaRi-Heart technology and treated by our FDA -approved LODOCO 0.5 mg tablets.” In June 2023, the U.S.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death.
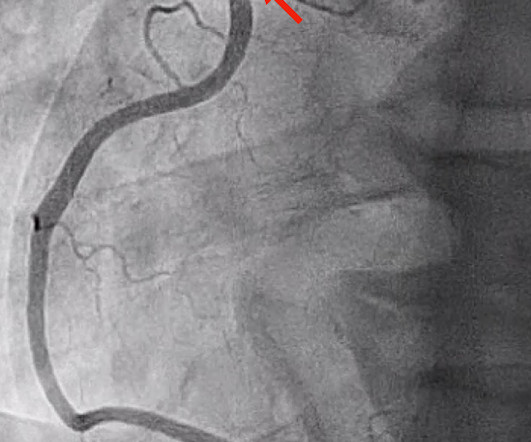
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardialinfarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Henry Ford Hospital. Henry Ford Hospital. Marcus, G. Harvard Medical School, Boston, Massachusetts, USA. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. Only beta-2 blockade (e.g., Hollander, J. de Lemos, J. Gibler, W. Gibler, W.
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. Answer: This is MINOCA -- MyocardialInfarction with Non-Obstructive Coronary Arteries. He had no further chestpain. The name is self-explanatory.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
However, data on whether a high-sensitivity HEART Pathway (hs-HP) are safe and effective is lacking.METHODS:An interrupted time series study was conducted at 5 North Carolina sites in 26 126 adult emergency department patients being investigated for possible acute coronary syndrome and without ST-segment–elevation myocardialinfarction.
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. You must record frequent serial ECGs for patients with chestpain. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. C harges and cost have no relation to each other in hospital billing. No, again, charges and cost have no relation to each other in hospital billing. A patient with chestpain: See the computer analysis.
Cardiology Board Review Question A 48-year-old female with no known medical history presents with acute substernal chestpain. Patients typically present with acute chestpain, shortness of breath, or syncope. The most common presenting symptom is acute substernal chestpain. What are the Symptoms?
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chestpain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardialinfarction, ventricular arrhythmia and sudden cardiac death.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. This is such a subtle ECG that I was worried that it had gone unnoticed, and, in fact, it did go unnoticed: His pain continued and his ECG was read as normal. He was admitted to the hospital for a "rule out."
A middle-aged woman had an acute onset of chestpain and dyspnea. The pain had almost resolved by the time an ECG was obtained in the ED: Here is the computer diagnosis What do you think? ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. It was not normal!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content