This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). One of the patients was lucky to have expert ECG interpretation by the Queen Of Hearts AI model. For 2 of the 3 patients — the cath lab was activated based on the ECG.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. Neverthelss, his anterior wall was saved and he had normal ejection fraction without heartfailure. What do you think?
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. The pain was unrelieved. It was not relieved by anything. What do you want to do?
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. I was told that the Queen of Hearts had called it OMI with high confidence. Also, we know the patient had a stent. Finally, the presentation is dyspnea, not chestpain. What do you think?
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chestpain. He had no h/o heartfailure. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. DBT was 120 minutes, pretty good for a Non-STEMI OMI.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. So the RCA was stented.
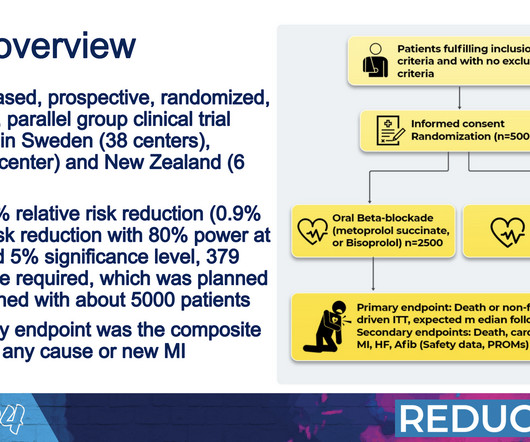
The findings call into question the routine use of beta blockers for all patients following a heart attack, which have stood as a mainstay of care for decades. Approximately 50% of heart attack survivors do not experience heartfailure. Over a median follow-up period of 3.5
No patient with chestpain should be sent home without troponin testing. All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. He now has regular appointments with the heartfailure team.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. Slow VT below the detection rate of the ICD lead to worsening heartfailure and low stroke volume.
She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
When OMI is captured in this early phase, there exists the highest amount of salvageable myocardium and least likelihood of heartfailure at hospital discharge. Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e.
It was stented. The patient would not have been diagnosed with acute coronary syndrome and would not have had an angiogram, would have been discharged (or perhaps had a stress test, which would be negative), and would be at great risk of another event, possibly resulting in death or heartfailure. Values: STE60V3 = 2.0,
A late middle-aged man presented with one hour of chestpain. This was stented. Heartfailure leading to death was related to all subclasses of PVC. He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. They end up with high mortality and needless heartfailure.
Written by Pendell Meyers A man in his 60s presented with acute chestpain. Total proximal LAD occlusion was found and stented at angiography soon after the ECG above. He was discharged home, but quickly bounced back 4 times within the next few months for worsening heartfailure.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content