This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). One of the patients was lucky to have expert ECG interpretation by the Queen Of Hearts AI model. In any case, the ECG is diagnostic of severe ischemia and probably OMI.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Dilation: The chambers of the heart expand, making the walls thinner. Both forms of enlargement may compromise the heart’s ability to pump blood efficiently, leading to further complications like heartfailure. What Causes an Enlarged Heart? Here are some of the most common causes: 1.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. How did the Queen of Hearts do on today's ECGs? The syncope lasted about 2-3 minutes according to his wife.
NOTE: It's important to correlate ongoing circumstances at the time that a prior tracing was done ( ie, Was the patient stable and asymptomatic — or were they having chestpain, an exacerbation of heartfailure, or some other ongoing process at the time the prior ECG was recorded? ).
Are you confident there is no ischemia? The heart rate is about 130 bpm. The heart rate could be compatible with that of a 2:1 conducted atrial flutter. Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Do you agree with this strategy?
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. Vitals were HR 58 BP 167/70 R20 sat 96%.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heartfailure for the last five years, and a prior ICD implantation five years ago. There is some ST-segment elevation in DII, DIII, aVF, V4-6.
The patient has heartfailure as a result of this event. A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chestpain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. No pericardial effusion. Alcohol intoxication?
ET Murphy Ballroom 4 Comparison of an "Inclisiran First" Strategy with Usual Care in Patients With Atherosclerotic Cardiovascular Disease: Results From the VICTORION-INITIATE Randomized Trial Targeting Weight Loss to Personalize the Prevention of Type 2 Diabetes Once-weekly Semaglutide in Patients with HeartFailure With Preserved Ejection Fraction, (..)
The chestpain quickly subsided. Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. NT-pro-BNP peaked at 4831, consistent with heartfailure. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia.
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chestpain (angina) or, in more severe cases, a heart attack.
This is one case where it made a difference: Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion Nevertheless, it is sometimes a fun academic exercise to try to predict the infarct artery: An elderly patient had onset of chestpain one hour prior. He called 911. Here is the prehospital ECG. What do you think?
She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? Does this patient have hypertension and/or heartfailure that has worsened? Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. LBBB may be the precipitating cause of the heartfailure syndrome, or may portend high mortality when identified in preexisting heartfailure.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. The Ratios of STE to S-wave: V1: 2.5/16 P EARL : Clinical correlation is KEY in this case.
This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. It appears that on occasion — J waves may be induced by ischemia ( thought to reflect an acute injury current from impending myocardial infarction ). But maybe not. Thelin et al.
This middle-aged patient has a remote history of cardiac surgery as a young child for a "heart murmur". She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. Exam was completely normal except for an irregular heart rate. She was on no medications.
A late middle-aged man presented with one hour of chestpain. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. Heartfailure leading to death was related to all subclasses of PVC.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. There is no evidence of infarction or ischemia. A cutoff of 1200 pg/ml for patients with a normal eGFR is very specific for heartfailure.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. Left BBB vi. Pathologic Q-waves viii.
They end up with high mortality and needless heartfailure. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L. The patient has acute persistent refrectory chestpain and elevated troponin.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. He presented to the emergency department for evaluation.
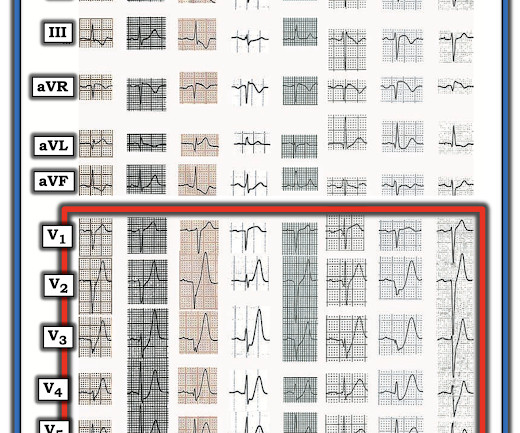
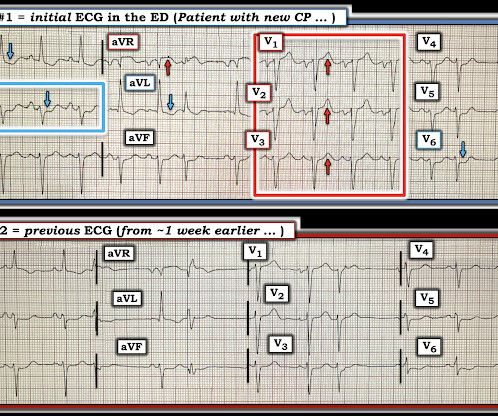
"Hi Steve wonder what you think of this ecg in a 60 yo woman w cp, known CAD" Presentation ECG (ECG 1): Here is her previous from one week prior when she presented with heartfailure and trops were "negative" (ECG 2): My response: "They both look like active ischemia. The previous ECG also shows active ischemia."
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Pendell Meyers A man in his 60s presented with acute chestpain. He was discharged home, but quickly bounced back 4 times within the next few months for worsening heartfailure. This distinction is further complicated because marked LVH may at times mask the ST-T wave changes of acute ischemia.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content