This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
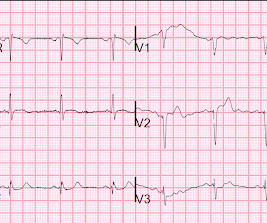
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
He had had several episodes of pain since onset; it was described as pressure-like and lasts about 5-15 minutes and resolves spontaneously. He had been pain free for about an hour. He had some "pre-diabetes ," but no h/o hypertension, no known family history of heartdisease, and he smokes about 1-2 cigarettes per day.
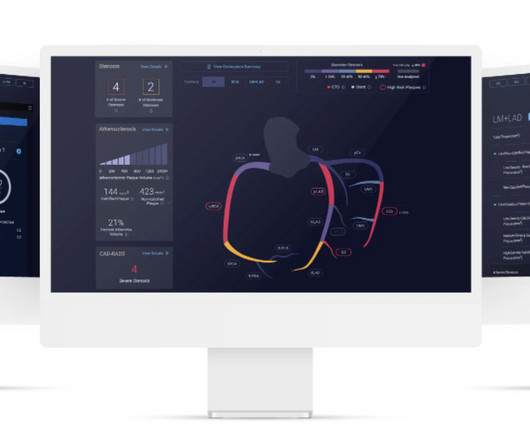
milla1cf Thu, 03/28/2024 - 07:00 March 28, 2024 — Cleerly , the company on a mission to create a new standard of care to aid in the diagnosis of heartdisease, shared findings from a study published online in the Journal of the American College of Cardiology: Cardiovascular Imaging on March 13, 2024. J Am Coll Cardiol. 2024.01.007.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. J Am Heart Assoc. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
The patient has acute chestpain. Here was my answer: "Not ischemia. If not HCM — some unusual form of cardiomyopathy might explain the findings in today's ECG (ie, muscular dystrophy; infiltrative heartdisease from amyloid or sarcoid; some unusual form of congenital heartdisease, etc. ).
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. Many of these patients have preexisting coronary and other forms of severe heartdisease. Smith's ECG Blog — Interpretation of a post-resuscitation ECG can be extremely challenging.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. Arbab-Zadeh, Heart Int 2012.
RVOT VT: A 40-something without past history presents with wide complex tachycardia and crushing chestpain Regular Wide Complex Tachycardia. A regular wide complex tachycardia in a young patient with no history of heartdisease is very likely to be AVRT. No , this requires inferior axis and LBBB morphology. 3 Pathways.
Are you confident there is no ischemia? The heart rate is about 130 bpm. The heart rate could be compatible with that of a 2:1 conducted atrial flutter. Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Do you agree with this strategy?
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heartdisease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. There is some ST-segment elevation in DII, DIII, aVF, V4-6.
She had a history of chronic respiratory disease and hypoxia, but hypoxia was no worse than normal. Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. The challenge is magnified when trying to assess BBB tracings for acute ischemia.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( It may also occur in patients with underlying coronary disease, cardiomyopathy, and/or with digoxin toxicity. Th e patient was hemodynamically stable in association with this rhythm.
But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. The Ratios of STE to S-wave: V1: 2.5/16 P EARL : Clinical correlation is KEY in this case.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heartdisease presented with chestpain that started on the morning of presentation at around 8am. Here is his triage ECG when he presented at 1657: What do you think?
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. He reported a history of “Wolf-Parkinson-White” and “heart attack” but said neither had been treated. Is there STEMI? Moffat, M.
This middle-aged patient has a remote history of cardiac surgery as a young child for a "heart murmur". She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. Exam was completely normal except for an irregular heart rate. She was on no medications.
Weren't you taught that "new tall T wave in V1" is concerning for ischemia, and so this is the opposite? Weren't you taught that concave morphology favors pericarditis? There is also new flattening of the T wave in V1 compared to prior.
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Her initial EKG is below. As a result — the main indication for treatment is to control symptoms.
She was noted to be tachycardic and her heart sounds were distant on physical exam. Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia.
Coronary Artery Disease (CAD) CAD, which involves the narrowing or blockage of coronary arteries due to plaque buildup, can reduce blood flow to the heart. This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Avoid excessive alcohol and drug use.
Within the complex umbrella of cardiovascular disease, CAD is a type of heartdisease that develops when the coronary arteries narrow and the heart cannot deliver enough oxygen-rich blood to the heart.
The ECG in Figure-1 was obtained from a 90-year old woman — who presented with a 2-to-3 day history of chestpain, that became worse on the day of admission. The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ).
One of the most common questions I get is, “ Do I need a stent to treat my heartdisease?” Ischemia Trial In an attempt to clarify this question, a similar trial was done called the Ischemia Trial, which had important differences to the Courage trial but again tried to answer a similar question 3.
No chestpain. Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). Later on during the night of his admission he had a short episode of chestpain that resolved with sublingual nitroglycerin. His vitals were initially normal.
There was no chestpain. She had no known heart condition. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). Even though the primary suspicion was not ischemic heartdisease, a CT angiogram was performed, and it revealed normal coronary arteries.
Knowledge of this fundamental pillar of biology should drive how cardiologists approach men and women being evaluated for the presence of significant coronary disease. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms.
In MSIMI (Mental Stress-induced Myocardial Ischemia) studies , mental stress activities like public speaking were evaluated for their impact on ischemia, measured via myocardial SPECT and vascular function (microvascular function, endothelial function). Combining behavioral and pharmacological treatment is most effective.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. This approach also reduces death from heartdisease and heart attacks by 41% compared to conventional approaches such as exercise stress testing 2.
The patient was a 70-something yo previously healthy male on no medications who presented to the ED with epigastric pain, onset over a few hours. He denied chestpain of any sort and his vitals were all normal. They cannot be assumed due to LV strain ( and they cannot be assumed to represent ischemia ).
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. LBBB is typically the result of preexisting hypertrophy, ischemic heartdisease, or cardiomyopathy.
As to ST-T wave changes in the 12-lead ECG — although some leads show T wave inversion (ie, in leads III, V3 and V4 ) — I did not think this looked acute in this 30-year old man without chestpain. Did the patient have some form of underlying heartdisease? No evidence of ischemia. What about the Repeat ECG?
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. h/o heartdisease (+1) 3.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chestpain. He said he had had three episodes of chestpain that day while urinating. No evidence for ischemia jumps out. ECG 1 What do you think?
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. He presented to the emergency department for evaluation.
He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. On presentation, he reported no chestpain or shortness of breath. Five days later, the patient was exercising when he developed chestpain at 19:30 which lasted for an hour.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content