This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." No further follow up is available.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. Exercise test would also have been reasonable. Read about "exercise induced cardiac troponin elevations" here.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
This ECG comes from Tom Bouthillet, who is devoted to good STEMI care, runs the EMS12lead ECG site , and who has also produced an outstanding iPhone/iPad/Android 12-lead ECG challenge App for learning to recognize subtle STEMI and to differentiate STEMIs and look alikes. There is 0.5 mm of ST depression in aVL.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. This was a machine read STEMI positive OMI. His ECG is shown below. Pretty obvious anterior current of injury. Readers of this blog can easily appreciate the hyperacute T waves in the precordium, clearest in V1-V4.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. LAD occlusion. Great case.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He was given aspirin and sublingual nitro and the pain resolved. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
He described the symptom as chest burning with occasional radiation into his throat and jaw. He first noticed it while exercising. The day of presentation, the pain woke him from sleep, which is why he decided to come in. The patient said his chestpain was 4/10, down from 8/10 on presentation.
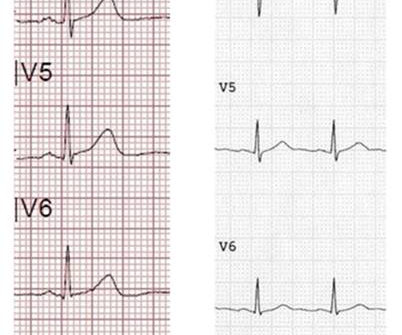
Furthermore, she denies any hydration since conclusion of exercise. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Smith comment : V5 and V6 are excessively discordant!!!!
The ECG in Figure-1 was obtained from a previously healthy middle-aged man — who while performing his regular exercise routine, developed "slight" chest discomfort and "palpitations". These symptoms persisted for over an hour, which led the patient to contact EMS.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI. See these similar cases: A man in his sixties with chestpain Why is there inferior ST elevation, and would you get posterior leads? is not known form the information we were provided.
His medical history is unremarkable except a similar pain occurred 4-5 times in the previous 3 months with less intensity, short duration, unrelated to exertion. He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. The pain was completely resolved after coronary intervention.
Sent by anonymous, written by Pendell Meyers A male in his teens presented with complaints of chest discomfort and dyspnea beginning while exercising but without obvious injury. He immediately stopped exercising and symptoms started to improve. He denied headache or neck pain associated with exertion. Pericarditis?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content