This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chestpain. The post ECG Cases 49 – ECG and POCUS for Dyspnea and ChestPain appeared first on Emergency Medicine Cases.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Ten days later the patient returned with worsening pleuritic chest.
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonaryembolism. She had been sitting doing work when she experienced "waves of chest tightness". She had been sitting doing work when she experienced "waves of chest tightness". Sats were 88%.
years, and the time from computed tomography pulmonary angiography (CTPA) diagnosis to interventional treatment averaged 2.8 ± 2.2 years, and the time from computed tomography pulmonary angiography (CTPA) diagnosis to interventional treatment averaged 2.8 ± 2.2 m, with an average age of 62.0 ± 16.0 m, with an average age of 62.0 ± 16.0
Genetic protein S (PS) deficiency caused by PROS1 gene mutation is an important risk factor for hereditary thrombophilia.Case introductionIn this case, we report a 28-year-old male patient who developed a severe pulmonaryembolism during his visit. The patient had experienced one month of chestpains, coughing and hemoptysis symptoms.
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonaryembolism. Acute pulmonaryembolism was confirmed on CT: The patient did well with treatment. What is the Diagnosis? This is a quiz.
The ECG is rather classic for pulmonaryembolism, and indeed this was a large acute PE. More on the ECG in pulmonaryembolism: The ECG in this patient has both precordial T-wave inversions AND T-wave inversion in lead III. this is highly suggestive of pulmonaryembolism. This is a classic S1Q3T3.
A 50-year-old man presented to the emergency department with symptoms of acute chestpain, dizziness, and headache. If the dissection extends into the aortic arch branches, ensuring adequate cerebral perfusion during surgery is crucial to preventing stroke. His blood pressure was 180/110 mmHg and heart rate was 100 bpm.
In this ECG Cases blog we look at 10 cases of patients with chestpain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. Patients with ACS and acute pulmonary edema 3. It was not relieved by anything.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The bedside echo showed a large RV (Does this mean there is a pulmonaryembolism as the etiology?) Here is his triage ECG: What do you think?
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. Only 5-13% of patients with chestpain and LBBB have MI; many fewer have coronary occlusion. Moreover, and importantly, there was sinus tach.
In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonaryembolism. Although it was technically difficult and the quality therefore leaves a lot to be desired, you can still make out RV dilation and septal flattening which is much more suggestive of pulmonaryembolism than OMI.
Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
Ken (below) is appropriately worried about pulmonaryembolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. Finally, the presentation is dyspnea, not chestpain. What do you think? Also, we know the patient had a stent.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. CT angiogram showed extensive saddle pulmonaryembolism. He had multiple cardiac arrests with ROSC regained each time.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. The CXR demonstrated no pulmonary edema. This latter part has been implicated in embolic CVA. The fall was not a mechanical etiology.
56 y/o male who presented with 12/10 severe chestpain starting at 3AM, radiating to his upper back. He had a history of pulmonaryembolism but was no longer on coumadin and states the pain is different. The patient was very hypertensive and had back pain, so they did a CT of his chest to rule out dissection.
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
Notice I did not say "pulmonaryembolism," because any form of severe acute right heart strain may produce this ECG. This includes, but is not limited to, PE, asthma/COPD exacerbation, hypoxic vasoconstriction from pneumonia, acute pulmonary hypertension exacerbation. What is the Diagnosis?
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. A new right bundle branch block in a sick patient with chestpain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonaryembolism.
My answer: "This is classic for PE, but it can also be present in any hypoxia due pulmonary hypoxic vasoconstriction and resulting acute pulmonary hypertension and acute right heart strain. The ECG of most patients with longstanding pulmonary disease show more r wave progression than I see in ECG #1. This is NOT Wellens.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
He said that his pain does not feel like his previous episode of pericarditis, and is not related to meals. He denied chestpain, shortness of breath, nausea, fever, chills, rashes, cough, and leg pain. Does subsegmental pulmonaryembolism matter? The ST/T ratio in V6, however, is slightly greater.
Written by Pendell Meyers, edits by Smith Two patients presented with acute chestpain/pressure. Chest x-ray was read as normal. CT pulmonary angiogram was negative for pulmonaryembolism. Two patients with chestpain. She had an acute LAD OMI in the process of reperfusion, see case below.
On his physical examination, cardiac and pulmonary auscultation was completely normal. As his pain was very severe, emergency physicians concerned of aortic dissection and ordered a thoracic CT scan. Bi-phasic scan showed no dissection or pulmonaryembolism. He has 40 packs-year of smoking history.
A male in his late 30's to early 40's presented with 24 hours of intermittent typical chestpain. This is known as McConnell's sign, and is described for PulmonaryEmbolism ; here we see it in right ventricular MI. The following ECG was recorded: There is an obvious acute inferior STEMI.
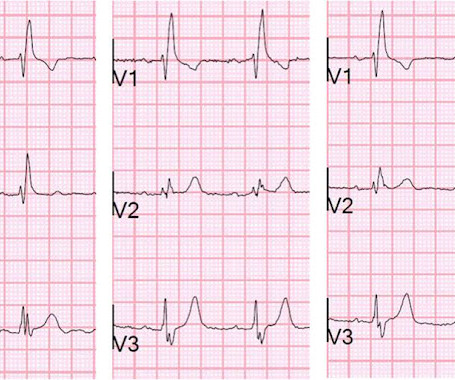
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. Patient 1 (ECG on the left) was a 45 year-old male, and patient 2 (ECG is on the right) was a 70 year-old male. But ECG #1 is not "normal".
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade.
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. Smith : This is classic for pulmonaryembolism (PE). Acute pulmonaryembolism was confirmed on CT angiogram: The patient did well. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
This study reports a rare case of concurrent AMI and pulmonary thromboembolism in a patient diagnosed with pancreatic cancer.Case presentationA 70-year-old woman presented with acute chestpain and ST-segment elevation myocardial infarction, prompting immediate percutaneous coronary intervention (PCI) with the deployment of a drug-eluting stent.
A 50-something man presented with worsening severe exertional chestpain which was just resolving as he had an ECG recorded in triage. By itself seeing this ECG pattern does not necessarily mean that the patient has a pulmonaryembolism. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know?
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He presented to the ED for evaluation chestpain. Pain was improved but not gone upon arrival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content