This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
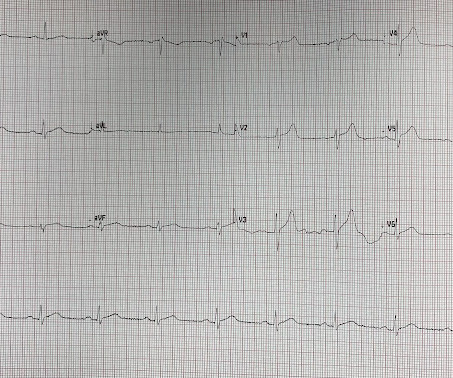
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
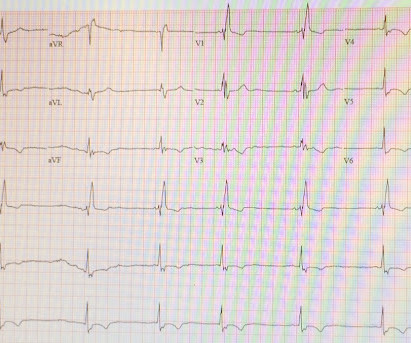
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
Angiogram: Severe 95% hazy distal LM Severe 80% ostial LAD, 100% occluded distal LAD thought to be due to distal embolization from the lesion in the proximal LAD. Post op chestpain Typical of post-op pericarditis (postpericardiotomy syndrome) There is ST Elevation in II > III, and STE in V3-5, but with flat T-wave.
A young otherwise healthy man presented with 4 hours of sharp 10/10 substernal chestpain. But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. This is a good sign for myocardial infarction and does not happen in pericarditis. BP was 160.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis Normal 0 false false false EN-US X-NONE X-NONE What do you think?
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. Unfortunately, we don't have those details.
In this ECG Cases blog we look at 10 cases of patients with chestpain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. CT angiogram showed extensive saddle pulmonary embolism. He had multiple cardiac arrests with ROSC regained each time.
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. A new right bundle branch block in a sick patient with chestpain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. Such an out-of-proportion STE is virtually never seen in pericarditis. STE in lead I and II are more subtle.
He denied fevers and chills, abdominal pain, chestpain, or SOB. Patients with completed, transmural infarct are also at risk for post-infarction regional pericarditis and myocardial rupture. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. Myocardial Rupture and Postinfarction Pericarditis.
Written by Pendell Meyers, edits by Smith Two patients presented with acute chestpain/pressure. Chest x-ray was read as normal. CT pulmonary angiogram was negative for pulmonary embolism. Two patients with chestpain. In a patient with chestpain — this is simply not a "normal" ST-T wave in lead V2.
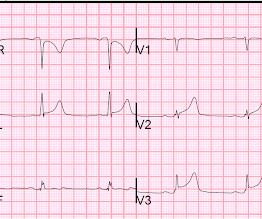
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” But ECG #1 is not "normal".
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
This is a very bold statement in a type 1 diabetic with very concerning sounding chestpain. The patient was treated with aspirin and a GI cocktail, which did not help the pain. Even if it is not atherosclerotic, young people can have embolic OMIs. The emergency physician consulted cardiology.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content