This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is also STE in lead III with reciprocal depression in aVL and I, as well as some subendocardial ischemia pattern with STD in V5-V6 and STE in aVR. Aslanger's is a combination of acute inferior OMI plus subendocardial ischemia, and due to the ischemia vectors , it has STE only in lead III. Moreover, there is tachycardia.
Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. Only 5-13% of patients with chestpain and LBBB have MI; many fewer have coronary occlusion. Moreover, and importantly, there was sinus tach.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. More detailed reviews of subendocardial ischemia, as well as acute ECG patterns that breach the typical presentation, can be found here: [link] [link] Imaging revealed no acute head, or spinal, injuries.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) An 80-something woman who presented with chestpain and dyspnea.
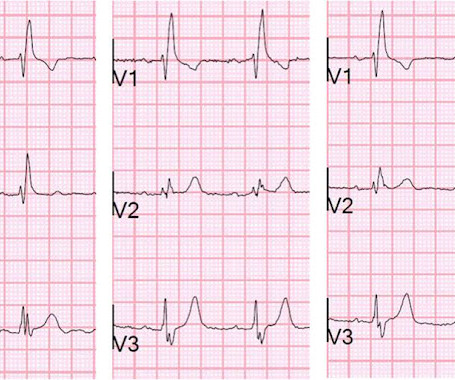
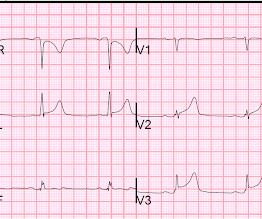
56 y/o male who presented with 12/10 severe chestpain starting at 3AM, radiating to his upper back. He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different. Here are V1-V3 from the last 3 ECGs: It is now clear that there is cardiac ischemia. Wraparound?
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
A young otherwise healthy man presented with 4 hours of sharp 10/10 substernal chestpain. The distal inferior apical LAD was cut off by distal embolization from LAD culprit. This is likely because 1) the ischemia to the inferior wall was only partial and 2) it reperfused quickly. It has been constant since then.
He denied fevers and chills, abdominal pain, chestpain, or SOB. Normal RBBB, no evidence of ischemia. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke. Patient stated his dry weight is around 85 kg. The emesis is non-bloody and non-bilious.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
A 40-something woman had sudden chestpain. However, by the time of the angiogram it had embolized distally, and had only done so after the right sided ECG was recorded. Figure-1: Initial ECG, obtained pre-hospital from this 40-ish year old woman with new-onset chestpain ( See text ). She called 911.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Blood Clots: An enlarged heart is more prone to developing blood clots, which can lead to stroke or pulmonary embolism.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Both of these are very suggestive of " No-Reflow ," or poor microvascular reperfusion due to downstream embolization of microscopic platelet-fibrin aggregates. hours when she called 911.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Evidence of acute ischemia (may be subtle) vii. Left BBB vi. Pathologic Q-waves viii.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
A 50-something man presented with worsening severe exertional chestpain which was just resolving as he had an ECG recorded in triage. Watch what happends as the heart recovers from its episode of ischemia. The ECG shows inferior ischemia. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know?
Written by Pendell Meyers A woman in her 40s presented with acute chestpain and shortness of breath. Smith : This is classic for pulmonary embolism (PE). Acute pulmonary embolism was confirmed on CT angiogram: The patient did well. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
Third, a slow motion segment showing delayed, brisk filling of the PDA due to dislodgment of a thrombus from contrast injection and distal embolization. A distal RCA lesion ( blue arrow ), Delayed brisk filling of an initially occluded PDA due to a thrombus dislodged during injection which embolized distally.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content