This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. The ECGs show a wide complex, irregularly irregular tachycardia. At this point, the patient had been symptomatic for almost 5 hours, appeared unwell with chestpain and diaphoresis.
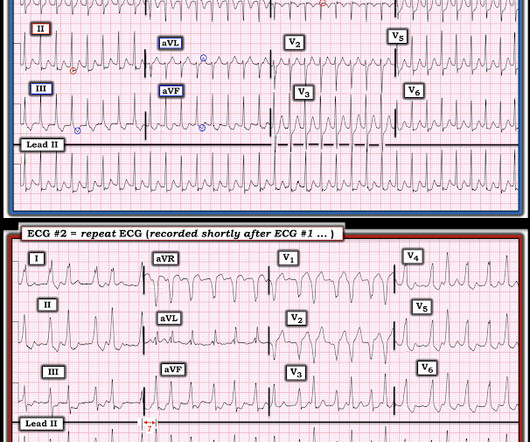
A 30-something presented with chestpain, palpitations, and SOB. The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." He has had similar symptoms for 4 years, but has never been evaluated.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Postablation chestpain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02) BACKGROUND:Inflammation may promote atrial fibrillation (AF) recurrence after catheter ablation. 2.02];P=0.89). 1.99];P=0.55).CONCLUSIONS:Colchicine
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. It was from a patient with chestpain: Note the obvious Brugada pattern. A rectal temperature was obtained which read 107.9 This patient ruled out for MI.
A late middle-aged man presented with one hour of chestpain. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. In multivariate analysis, serum potassium level was negatively and age positively related to ventricular tachycardia. Most recent echo showed EF of 60%.
POTS stands for postural orthostatic tachycardia syndrome. Let’s call it Postural Orthostatic Tachycardia Syndrome – that’s not really a diagnosis – it’s just a medical jargon filled term for what the patient has just told us. What is POTS? When you examine them, the heart rate can be found to be excessively fast.
2 weeks Here is the final electrophysiology note: It is unclear what precipitated his motor vehicle collision. ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. BP:143/99, Pulse 109, Temp 37.2 °C
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Electrophysiologic studies were performed in selected patients only as clinically appropriate.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chestpain. He said he had had three episodes of chestpain that day while urinating. So the most likely rhythm in ECG 1 is ectopic atrial tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content