This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." The initial troponin I was elevated at 0.75
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. Pain better still. What do you think the echocardiogram shows? NTG drip started.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think? Do NOT use them.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. He presented to the Emergency Department with a blood pressure of 111/66 and a pulse of 117. He had this ECG recorded. Troponins peaked at 0.275 ng/ml.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
3 hours prior to calling 911 he developed typical chestpain. 1.196 x STE60 in V3 in mm) + (0.059 x computerized QTc) - (0.326 x RA in V4 in mm) Third, one can do an immediate cardiac ultrasound. Medics gave him nitroglycerine sublingual and his pain resolved. greater than 23.4 is likely anterior STEMI).
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. Bedside echocardiogram showed hypokinesis of the mid to distal anterior wall and apex.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. If detected early by ultrasound, the patient can be saved. There was some SOB. He had walked into the ED (did not use EMS). 3) Oliva et al. (3)
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. On medic arrival, she walked out of the house in no distress, but was diaphoretic.
No chestpain. His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. An echocardiogram showed no hemopericardium, but D oppler showed a new small ventricular septal defect with left to right shunting. There was some SOB.
Inflammation of pericardium as inflammation elsewhere can be painful and cause chestpain. But pericardial effusion can build up slowly without much pain. Sometimes mild pericardial effusion may be detected by an echocardiogram done for other causes.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. His echocardiogram showed normal wall motion.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. See this case: what do you think the echocardiogram shows in this case?
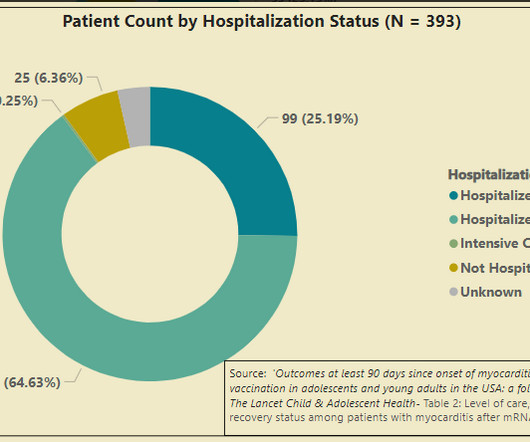
The current study should dispel the ludicrous notion that clinical myocarditis - a disease entity that comes to light when you have chestpain because cells in your heart are dying — is mild. The CDC study published in Lancet on previously healthy 12-29 years old’s is a survey-based study.
History : An extremely elderly patient who lived independently presented with acute "oppressive" chestpain 7/10 in severity that was not positional, pleuritic, or reproducible. These ultrasounds confirm LAD occlusion. What's the story?" Exam was benign and VS were normal.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Smith comment: This patient did not have a bedside ultrasound. In fact, bedside ultrasound might even find severe aortic stenosis. What should be done?
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. orthostatic vitals b.
Patients who present with chestpain or cardiac arrest and have an ECG diagnostic of STEMI could have myocardial rupture. 5 of 6 presented with chestpain and an ECG indicating reperfusion therapy, but were detected by bedside ultrasound. Obviously, administration of heparin and/or lytics is hazardous.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. A bedside POC cardiac ultrasound was done: Findings: Decreased left ventricular systolic function. BP:143/99, Pulse 109, Temp 37.2 °C
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Echocardiogram showed inferior hypokinesis. Troponin was rising when last checked, 8928 ng/L.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content