This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. Due to the chestpain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. He had associated nausea, vomiting, and dyspnea.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). Patient #1 in today's post did not get expert ECG interpretation.
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. There is sinus tachycardia. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. See this post: What do you think the echocardiogram shows in this case?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
This 54 year old patient with a history of kidney transplant with poor transplant function had been vomiting all day when at 10 PM he developed severe substernal crushing chestpain. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock. He had this ECG recorded. Are the lungs clear?
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 1 remained in the hospital overnight. It was stented.
Advanced cardiac imaging especially in atypical presentations, can aid in early diagnosis.Case:A 59 year-old man with history of biopsy-proven pulmonary sarcoidosis presented with non exertional chestpain for 2 months. EKG, cardiac enzymes, and Initial echocardiogram(TTE) was unremarkable.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Hopefully a repeat echocardiogram will be performed outpatient. RBBB in blunt chest trauma seems to be indicative of several RV injury. No cardiac MRI was done.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. A rapid echocardiogram was performed, revealing an ejection fraction of 20% with thinning of the anterior-apical walls. What is the rhythm? Smith : Are they P-waves?
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
They were recorded 12 minutes apart: "Hey Steve, 30-something with one week of chestpain, mostly right-sided, better with sitting up.": Get an emergent contrast echocardiogram. This history of a week of constant chestpain is also much more suggestive of myocarditis. What do you think? flat ST segment in V4 2.
Case 1 A middle aged woman presented with acute chestpain and shortness of breath, unclear time since onset, and likely with episodic symptoms off and on throughout the day. Echocardiogram: EF 50%, akinesis of mid-apical anteroseptal, inferior, and inferoseptal myocardium. Submitted by anonymous, written by Pendell Meyers.
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Now the patient is in sinus tachycardia. She had an echocardiogram which was normal.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. See this case: what do you think the echocardiogram shows in this case? A normal PR interval.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. Severe Tachycardia Acute Coronary Syndrome (obstructive coronary disease) a. This results in Type I MI.
The pneumothorax was expanded with a chest tube At 17 hours, another ECG was recorded: It is now much less dramatic and has the morphology of Type 2 Brugada The hs troponin I peaked at 6500 ng/L -- this strongly suggests myocardial contusion. An echocardiogram was done. Sinus Tachycardia ( common in any trauma patient. ).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. We can see enough to make out that the rhythm is sinus tachycardia. It was not worse with exertion or relieved by rest.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
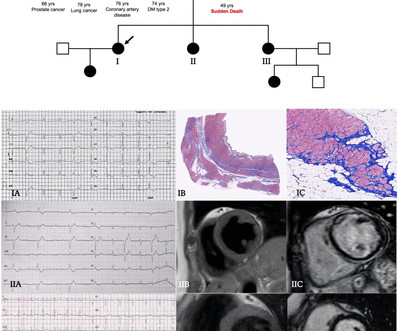
Twenty-one (41%) had normal echocardiogram, 13 (25%) a hypokinetic non-dilated cardiomyopathy (HNDC) and 17 (33%) a dilated cardiomyopathy (DCM). Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chestpain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%).
However, an echocardiogram is a different test, also conducted for heart activity. If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. BP:143/99, Pulse 109, Temp 37.2 °C
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD.
Patients who present with chestpain or cardiac arrest and have an ECG diagnostic of STEMI could have myocardial rupture. 5 of 6 presented with chestpain and an ECG indicating reperfusion therapy, but were detected by bedside ultrasound. Obviously, administration of heparin and/or lytics is hazardous.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Most physicians will automatically be worried about these symptoms.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
He denied chestpain. A Chest X-ray did not show pulmonary edema. This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. It is correct that he did not have chestpain, but we must remember that fully 1/3 of full blown STEMI do not present with chestpain.
He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. On presentation, he reported no chestpain or shortness of breath. Five days later, the patient was exercising when he developed chestpain at 19:30 which lasted for an hour. Or both?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content