This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Upon questioning patient, he denies having any chestpain or chest tightness of any sort. In the absence of chestpain and negative troponin , it appears less likely that he is having acute coronary syndrome though EKG appears concerning. Pericarditis would be even more unlikely in someone without chestpain.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. First troponin I returns at 48 ng/L ECG 5 143 min No significant change ECG 6 261 min Same hs Troponin I profile (peaked at 1849): Formal Echocardiogram SUMMARY The estimated left ventricular ejection fraction is 74 %.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. She has done quite a bit of research on the topic. Given that chestpain is resolving at the time ECG #2 was recorded — this supports the concept of dynamic ST-T wave changes in this patient.
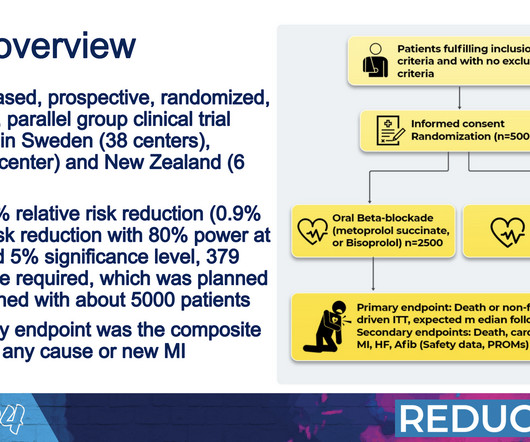
However, researchers said that the clinical trials that led to this routine use of beta blockers were conducted before the advent of many newer procedures that are now widely used to open blocked arteries. The researchers plan to separately analyze outcomes related to quality of life and sexual health.
I remember Allie well from her days in the Research volunteer program at Hennepin. A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. It was from a patient with chestpain: Note the obvious Brugada pattern.
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. He subsequently describes having sharp chestpain over the next few weeks. The pain resolved a few weeks later. He emphatically denies any history of cardiopulmonary disease.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Echocardiogram showed inferior hypokinesis. Just look at all the research based on this !
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content