This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
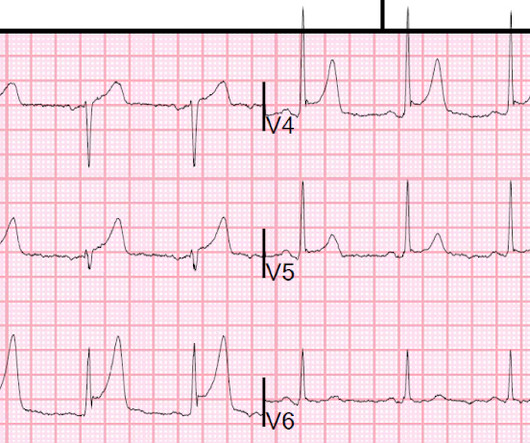
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). Patient #1 in today's post did not get expert ECG interpretation.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." The initial troponin I was elevated at 0.75 Lobo et al.
No patient with chestpain should be sent home without troponin testing. An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. An echocardiogram showed an EF of 20-25%. Three months later, he had a follow up appointment for a reassessment of his LV function.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Formal Echocardiogram: Normal left ventricular size and wall thickness.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Wellen's syndrome is a Reperfusion syndrome.
He had no chestpain. The computer read is: **Acute MI ** The protocol for prehospital activation in the EMS system that this patient presented to requires 2 elements: 1) Chestpain 2) A computer read of **Acute MI ** Only 1 of 2 was present, so there was no prehospital activation. The patient was transported to the ED.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. On echocardiogram, there was a 40% ejection fraction with anterior wall motion abnormality. This patient had continued and ongoing pain. His ECG was repeated at this point: This shows a well developed anterior STEMI.
Hopefully a repeat echocardiogram will be performed outpatient. ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. 1900: RBBB and LAFB are almost fully resolved.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Gottlieb SO, et al.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. The 1st “lesson” is, “All bets are off” — when an adult of any age presents to the ED with new-onset chest discomfort. Regional wall motion abnormality-distal inferior wall.
A 40 something otherwise healthy man presented with substernal chestpain. Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. What do you think? This ECG is DIAGNOSTIC of acute LAD Occlusion.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. See this case: what do you think the echocardiogram shows in this case?
Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. He did not remember whether he had experienced any chestpain. Two subsequent troponins were down trending. Within a few days, the patient was extubated and was neurologically intact.
Case 1: The outcome of this case is at the far bottom. He complained of severe chestpain and was extremely agitated, so much so that he was throwing chairs in triage. In any case, the patient needs at a minimum serial ECGs and perhaps a formal echocardiogram. His chestpain resolved.
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. At midnight.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think? Do NOT use them.
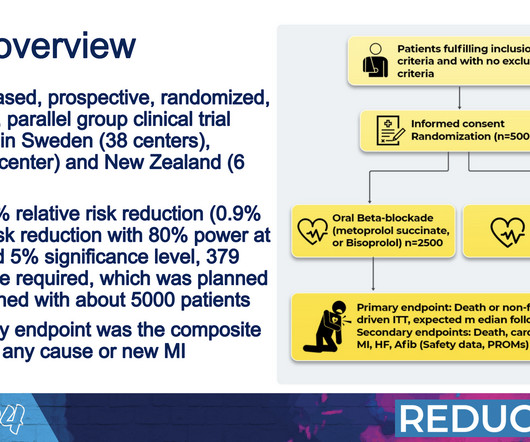
All patients had an ejection fraction of 50% or higher as assessed with an echocardiogram performed within one week of their heart attack. While this unblinded approach could potentially introduce bias, researchers said that this was not likely to have an effect on outcomes such as death and heart attacks.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. Although the patient has had pain for 4 days, could the artery have fully occluded only within hours? There was some SOB. Very unlikely. Raitt et al.) [and
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. such Q-waves are associated with larger MI and worse outcomes (2. There was some SOB. He had walked into the ED (did not use EMS). Obviously there is MI.
History : An extremely elderly patient who lived independently presented with acute "oppressive" chestpain 7/10 in severity that was not positional, pleuritic, or reproducible. Because of occasional catastrophic outcomes in patients with transient STEMI, I recommend that it be managed just like a persistent STEMI.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). These premonitory symptoms were negative predictors of adverse outcomes in EGSYS.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Echocardiogram showed inferior hypokinesis. Troponin was rising when last checked, 8928 ng/L.
Written by Pendell Meyers, few edits by Smith A woman in her 70s was woken from sleep by midsternal chestpain radiating to left arm with nausea. Echocardiogram: EF 42% Moderate hypokinesis of the mid anterolateral and apical lateral myocardium Final diagnosis by the cardiologist was "STEMI" despite never meeting STEMI criteria.
Written by Pendell Meyers A man in his 60s presented with acute chestpain. Long term outcome is not available. == MY Comment, by K EN G RAUER, MD ( 2/1/2025 ): == We need to learn from cases like today's. Here is his triage ECG: What do you think? There is sinus rhythm with clear LVH. 4 days later: Continued reperfusion.
He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. On presentation, he reported no chestpain or shortness of breath. Five days later, the patient was exercising when he developed chestpain at 19:30 which lasted for an hour.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content