This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). Despite active CP — cath lab activation was deferred and this patient was transported to a local hospital without PCI capability.
He was intubated in the field and sedated upon arrival at the hospital. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. He did not remember whether he had experienced any chestpain. At his family's request, he was transferred to a hospital closer to his home to continue care.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
He was treated for infection and DKA and admission to hospital was planned. While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest.
After 24 hours, the patient was readmitted to the hospital with chestpain and troponin elevation, without ECG changes. A transthoracic echocardiogram (TTE) revealed a mobile mass on the right coronary cusp of the aortic valve ( figure 1 , ). The patient was discharged and apixaban was restarted 10 hours later.
The medics stated he had been nauseated and diaphoretic, but he did not have any chestpain or SOB. And especially suspect Old MI when the patient gives a history of MI and has no chestpain or SOB. Case continued The patient underwent an emergency formal echocardiogram and it was unchanged. Learning Points: 1.
Our report describes two cases of SVS treated with endocardial ablation to improve LVOTO.Case reportCase 1: A 74-year-old female patient with angina and syncope was admitted to the hospital and diagnosed with SVS by transthoracic echocardiogram. After RFA was performed, the patient's symptoms significantly improved.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. He had been seen several weeks ago at an outside hospital for a similar issue and had been discharged home, presumably after unremarkable workup.
He was admitted to the hospital for evaluation of these symptoms — but no ECG was done at that time. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The proximal LAD is now widely patent.
He was admitted to our hospital with issues of chestpain, shortness of breath and heart palpitations without any obvious inducement. Figure 1 Transthoracic echocardiogram. (A) He had no medical history of myocardial infarction (MI). A 12-lead ECG indicated sinus rhythm with a heart rate of 78 bpm.
While in the hospital, he had witnessed ventricular fibrillation (VF) arrest for which he received external defibrillation. An echocardiogram showed newly reduced left ventricular ejection fraction of 30-35%.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 1 remained in the hospital overnight.
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
3 hours prior to calling 911 he developed typical chestpain. When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia. Pain was typical for MI (substernal, not postional or sharp, resolved with NTG) b. Transient ST elevation is very hazardous.
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. The echocardiogram shows a preserved left ventricular ejection fraction (LVEF) of 55% with marked basal and mid inferolateral and basal anterolateral hypokinesia. The first ECG (10h14) showed TWI in inferior leads."
No patient with chestpain should be sent home without troponin testing. An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. An echocardiogram showed an EF of 20-25%. Here is the post-cath EKG: There is no change. The LV aneurysm morphology persists.
However, an echocardiogram is a different test, also conducted for heart activity. Patients use them to observe their heart activity by themselves when they are not in the hospital. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. ECG and EKG refer to the same thing.
Yes, COVID-19 symptoms can resemble a heart attack, including chestpain, shortness of breath, and changes in echocardiogram or EKG. Myocarditis symptoms can also mimic a heart attack, and small blood clots may cause pain. Can COVID-19 symptoms mimic a heart attack?
Hopefully a repeat echocardiogram will be performed outpatient. ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. 1900: RBBB and LAFB are almost fully resolved.
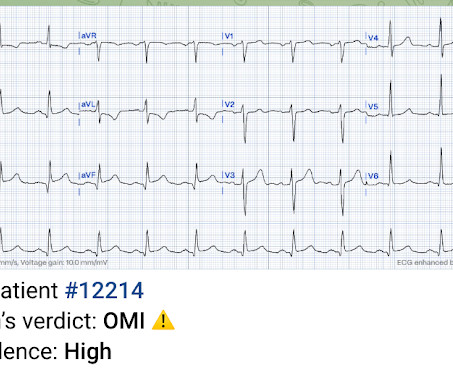
On the other hand — the ST elevation seen in lead V1 is perfectly consistent with LVH and LV "strain" ( ie, The shape of this ST-T wave in lead V1, in association with the deep S wave in this lead — is a mirror-image opposite picture of the typical expected appearance of LVH with "strain" in a lateral chest lead ).
The relationship between low RHR and CI has yet to be described.Purpose:We hypothesize that resting sinus bradycardia (low RHR) could be a predictor of chronotropic incompetence and reduced exercise capacity.Methods:The derivation cohort consists of 201 patients with normal Bruce protocol treadmill stress echocardiogram. x age in years).Results:The
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. He was admitted to the hospital for a "rule out." On echocardiogram, there was a 40% ejection fraction with anterior wall motion abnormality. His first troponin was normal. The peak troponin I was over 100.
The patient was promptly admitted to the hospital for further evaluation. Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. An initial electrocardiogram (ECG) is provided below. What do you think? What is the rhythm?
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. This is her pre-hospital ECG: This is her first ECG in the ED: What do you think? While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 hours of substernal chest pressure. She had zero CAD risk factors. It is equivalent to a transient STEMI.
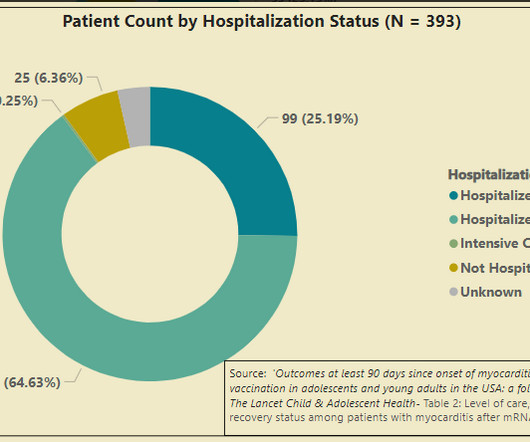
The current study should dispel the ludicrous notion that clinical myocarditis - a disease entity that comes to light when you have chestpain because cells in your heart are dying — is mild. So, of the 989 cases of myocarditis that were identified via VAERS, there is information on hospitalization status for 519 of them.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. See this case: what do you think the echocardiogram shows in this case?
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. Echocardiogram findings (pre-procedure) 1. A 12 Lead ECG was captured on her arrival.
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. She had an echocardiogram which was normal. She reported a prior history of SVT and has previously performed vagal maneuvers at home with symptom resolution. Her initial EKG is below.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Del Rosso A, et al.
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. The vast majority of cases of vaccine myocarditis requires hospitalization for monitoring for deterioration. He subsequently describes having sharp chestpain over the next few weeks.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. The patient was given furosemide and admitted to the hospital. BP:143/99, Pulse 109, Temp 37.2 °C C (99 °F), Resp (!)
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Echocardiogram showed inferior hypokinesis. Troponin was rising when last checked, 8928 ng/L.
He denied chestpain. In this study of consecutive patients with LBBB who were hospitalized and had an echocardiogram, a QRS duration less than 170 ms (n = 262), vs. greater than 170 ms (n = 38), was associated with a significantly better ejection fraction (36% vs. 24%). And here the lines show the offset.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content