This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
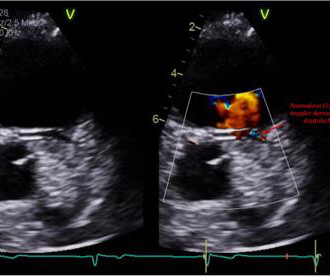
Clinical introduction A man in his 40s with a history of hyperlipidaemia presented with intermittent, dull left-sided chestpain for 2 weeks that was not consistently exertional. Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. A transthoracic echocardiogram was performed ( figure 1 ).
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Formal echocardiogram: Systolic function is at the lower limits of normal. Three patients with chestpain and “normal” ECGs: which had OMI?
The echocardiogram showed normal cardiac structure and function, however, there was a concern for possible anomalous origin of the left coronary artery. Treadmill exercise stress test showed excellent functional capacity without exercise-induced chestpain or ischemic ECG changes.
Yes, COVID-19 symptoms can resemble a heart attack, including chestpain, shortness of breath, and changes in echocardiogram or EKG. Myocarditis symptoms can also mimic a heart attack, and small blood clots may cause pain. Exercise should be reintroduced gradually, ruling out structural abnormalities first.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. LAD occlusion. Great case.
No patient with chestpain should be sent home without troponin testing. On this visit, he expressed worsening exercise tolerance, new orthopnea, and he told his provider that the omeprazole did not relieve any symptoms. An echocardiogram showed an EF of 20-25%. His BP was now 82/68, and his HR was 112.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
Echocardiogram: Estimated left ventricular ejection fraction, lower limits of normal; 45-50%. In my experience — sinus tach rarely exceeds 170/minute in a non-exercising adult patient. Tele Monitor: Normal sinus rhythm throughout, no ectopic atrial or ventricular beats. Regional wall motion abnormality-inferior/inferoseptum: akinetic.
Chest X-Ray A chest X-ray is often the first imaging test conducted, as it can reveal whether the heart is enlarged and by how much. Echocardiogram An echocardiogram uses sound waves to produce a detailed image of the heart, allowing doctors to see the size of the heart chambers and how well the heart is pumping blood.
Background:Cardiac output reserve and exercise capacity are strong predictors of life expectancy. Chronotropic incompetence (CI) is the inability to reach an age appropriate maximum heart rate with exercise. CI reduces cardiac output reserve and exercise capacity, both of which increase all-cause mortality risk. x age in years).Results:The
His medical history is unremarkable except a similar pain occurred 4-5 times in the previous 3 months with less intensity, short duration, unrelated to exertion. He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. He has 40 packs-year of smoking history.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content