This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Formal echocardiogram: Systolic function is at the lower limits of normal. Three patients with chestpain and “normal” ECGs: which had OMI? Which were normal?
Chest X-Ray A chest X-ray is often the first imaging test conducted, as it can reveal whether the heart is enlarged and by how much. Echocardiogram An echocardiogram uses sound waves to produce a detailed image of the heart, allowing doctors to see the size of the heart chambers and how well the heart is pumping blood.
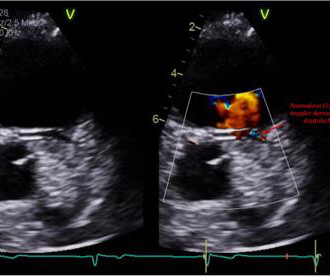
Electrocardiogram in clinic showed sinus arrhythmia with early repolarization and no ischemic changes. The echocardiogram showed normal cardiac structure and function, however, there was a concern for possible anomalous origin of the left coronary artery. Invasive coronary angiography ruled out luminal narrowing or dynamic compression.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Formal echocardiogram showed normal EF, no wall motion abnormalities, no pericardial effusion.
Case presentation:A 64-year-old man presented with one day of chestpain. Electrocardiogram (EKG) was unremarkable. Transthoracic echocardiogram (TTE) showed an ejection fraction (EF) of 40% and a moderate-large pericardial effusion with signs of tamponade. He was decannulated from ECMO on day 10.
However, an echocardiogram is a different test, also conducted for heart activity. An electrocardiogram is a machine used to record the heart's electrical activity. If you experience shortness of breath, chestpain, fatigue, or irregular heartbeat, you will be recommended an ECG test to check if you have heart inflammation.
Yes, COVID-19 symptoms can resemble a heart attack, including chestpain, shortness of breath, and changes in echocardiogram or EKG. Myocarditis symptoms can also mimic a heart attack, and small blood clots may cause pain. Can COVID-19 symptoms mimic a heart attack?
The attending provider wrote “Agree with electrocardiogram interpretation”. No patient with chestpain should be sent home without troponin testing. An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. An echocardiogram showed an EF of 20-25%.
He has never had any chestpain. Echocardiogram is indicated (Correct) C. Start aspirin and Plavix Correct answer: (B) (B) Echocardiogram is indicated. Explanation: Shown electrocardiogram suggests left ventricular hypertrophy. Shown electrocardiogram suggests left ventricular hypertrophy.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
An initial electrocardiogram (ECG) is provided below. Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. The patient was promptly admitted to the hospital for further evaluation. What do you think? What is the rhythm?
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardial infarction. International Journal of Cardiology Heart & Vasculature Case A 40-year-old man presents with excruciating back pain which has started 1 hour ago. He denies taking any medication.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Patel DJ, et al.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. See this case: what do you think the echocardiogram shows in this case? Harhash AA, Huang JJ, Reddy S, et al.
A 40 something otherwise healthy man presented with substernal chestpain. Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. What do you think? This ECG is DIAGNOSTIC of acute LAD Occlusion.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. It was from a patient with chestpain: Note the obvious Brugada pattern. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade.
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. He subsequently describes having sharp chestpain over the next few weeks. The pain resolved a few weeks later. He emphatically denies any history of cardiopulmonary disease.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content