This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This is an interesting case for your students who want to delve into dysrhythmias with an eye on detail. I will start the discussion by admitting that I am not an expert of electrophysiology or complex dysrhythmias. I hope some of our dysrhythmia Gurus will delve into the rhythm and maybe even provide laddergrams.
This is an interesting case for your students who want to delve into dysrhythmias with an eye on detail. I will start the discussion by admitting that I am not an expert of electrophysiology or complex dysrhythmias. I hope some of our dysrhythmia Gurus will delve into the rhythm and maybe even provide laddergrams.
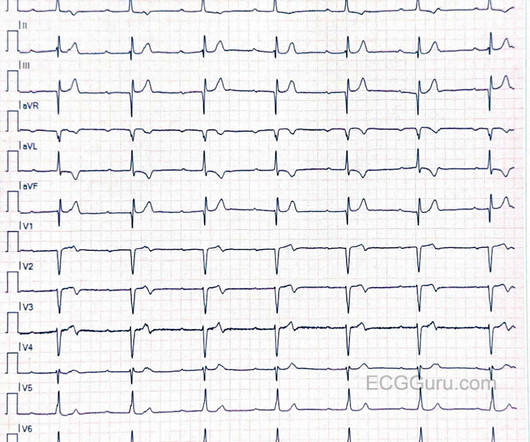
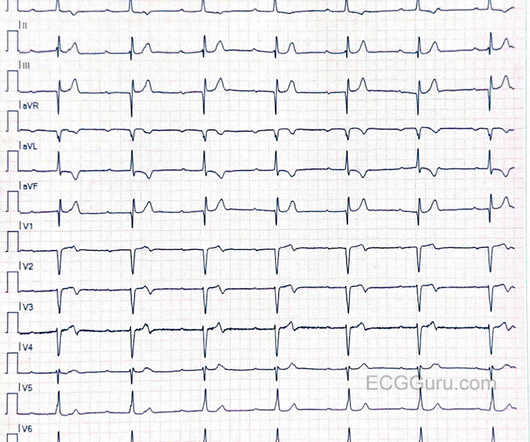
This case was sent by Dr Avinash Krishnamurthy, a fine emergency medicine resident from Australia Cairns base hospital Case : An adolescent male had a mechanical fall and injured his left shoulder and arm. There was apparently no syncope and he had no bony injuries, but he did complain of left sided chestpain. What is it?
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. At this point, the patient had been symptomatic for almost 5 hours, appeared unwell with chestpain and diaphoresis. Thus, the patients rhythm is atrial fibrillation with WPW.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chestpain. Upon EMS arrival the patient appeared acutely ill and complained of chestpain. Is it sinus or is it a supraventricular dysrhythmia?
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
I also believe that we physicians and medics are eager to treat dysrhythmias, and we want to see them even when they are not there. Henry Ford Hospital. Henry Ford Hospital. Dilated pupils and hypertension are a strong clue to sympathetic overload, but don't forget anticholinergic syndromes, including tricyclics! Marcus, G.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. He was prescribed apixaban.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 hours of substernal chest pressure. She had zero CAD risk factors. It is equivalent to a transient STEMI.
A late middle-aged man presented with one hour of chestpain. Could the dysrhythmias have been prevented? Severe hypokalemia in the setting of STEMI or dysrhythmias is life-threatening and needs very rapid treatment. Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III.
He was admitted for monitoring, as his risk of a ventricular dysrhythmia as cause of the syncope is high ( very high due to HFrEF and ischemic cardiomyopathy ). He denied chestpain or dyspnea throughout. Unfortunately, this option might not be available for pre-hospital tracings. See text ).
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. But adenosine only lasts for seconds, and if the dysrhythmia recurs, then the adenosine is gone. Prevent the initiation of the dysrhythmia -- this can be done with a beta blocker by prenenting PACS 2.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Del Rosso A, et al.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. The patient was given furosemide and admitted to the hospital. BP:143/99, Pulse 109, Temp 37.2 °C C (99 °F), Resp (!)
Sinus tach is often misinterpreted as a dysrhythmia. With OMI, all you know is that your patient has some nonspecific chestpain, SOB, shoulder pain etc. They often have good ejection fraction and tolerate the dysrhythmia quite well. As noted ECG #4 was obtained later in this patient's hospital course.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content