This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc. She received PCI with 2 drug-eluting stents in overlying fashion.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chestpain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
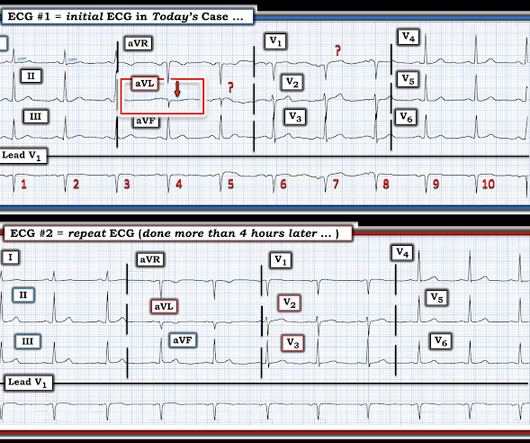
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). The patient was still with ongoing chestpain at the time ECG #1 was done.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No There are well-formed Q-waves 3.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. mV compared to 0.05-0.1
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." The following ECG was obtained.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The operator documented thoughtful consideration of risks and benefits of stent placement. Unfortunately, a few hours later the patient complained of recurrent chestpain. She took an oxycodone and called EMS.
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis?
It was opened and stented. The reason the initial ECG is so concerning — is that it already suggests high likelihood of OMI ( = O cclusion-based MI ) in this 50-ish year old man who presents with a 2-hour history of new chestpain. Formal bubble contrast echo: The estimated left ventricular ejection fraction 57%.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss.
A 40-something woman had sudden chestpain. He did, found the true culprit, and went back in to stent it. Figure-1: Initial ECG, obtained pre-hospital from this 40-ish year old woman with new-onset chestpain ( See text ). She called 911. But which myocardial walls are affected? Learning Points: 1.
Opened and stented. Instead, in a patient with new chestpain and hyperacute inferior lead T waves — this picture that we see in lead V3 suggests associated posterior OMI until proven otherwise. Our definition of hyperacute T-waves is that their AUC in proportion to the QRS amplitude is greater than normal T-waves.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. The last echocardiography 12 months ago showed HFmrEF.
Triage documented a complaint of left shoulder pain. See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. Here is the angiogram after stent placement. At midnight.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think?
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Past medical history includes coronary stenting 17 years prior.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
A late middle-aged man presented with one hour of chestpain. This was stented. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III. He had recently had a NonSTEMI.
Written by Willy Frick A young woman with a history of paroxysmal nocturnal hemoglobinuria presented with acute substernal chestpain. The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. Smith : The cath lab should be activated now!
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. After stent placement: The vessel is now open with TIMI 3 flow, although it is diffusely diseased and the middle segment is ectatic.
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." This is a very bold statement in a type 1 diabetic with very concerning sounding chestpain. Several hours passed with no documentation as to the reason for delay.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. Galiuto, L., Yoshida, T.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content