This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
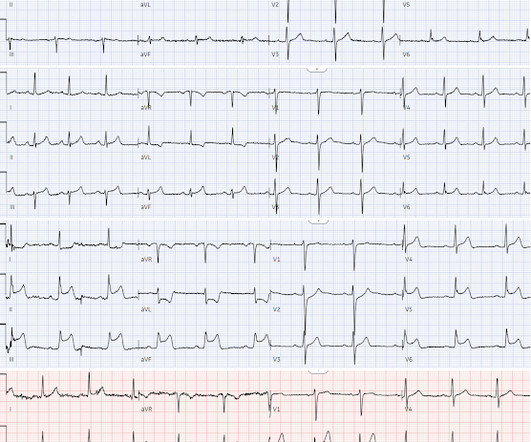
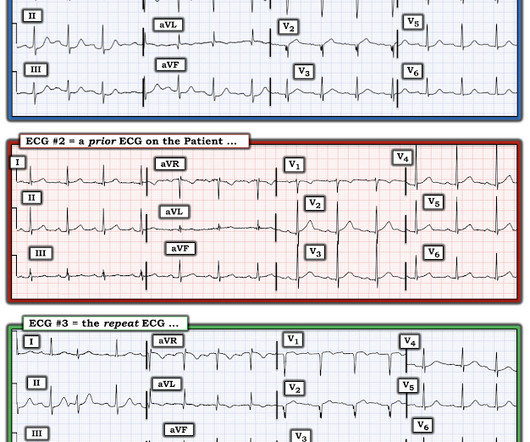
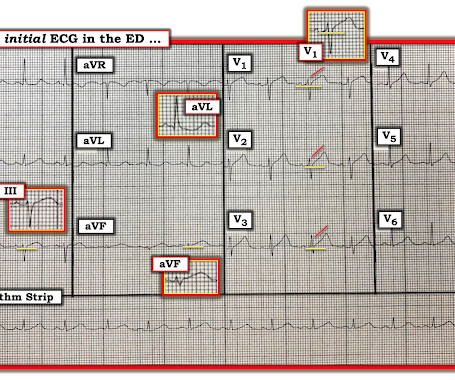
Written by Jesse McLaren A 45-year-old presented with 24 hours of intermittent chestpain. On it’s own this is nonspecific, but in the right context this could be diagonal occlusion (if active chestpain) or infero-posterior reperfusion (if resolved chestpain). #2 Can you guess the sequence?
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Written by Jesse McLaren Four patients presented with chestpain. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
Submitted by Dr. Dennis Cho (@DennisCho), written by Jesse McLaren A 70-year-old with no cardiac history presented with 2 hours of chestpain radiating to the neck, associated with shortness of breath. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI?
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). In STEMI, they are generally upright and large in proportion to the QRS. So this argues against acute STEMI.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). But it does not meet STEMI criteria and it was not initially recognized.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Anxiety is a common cause of chestpain with tachycardia.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chestpain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin.
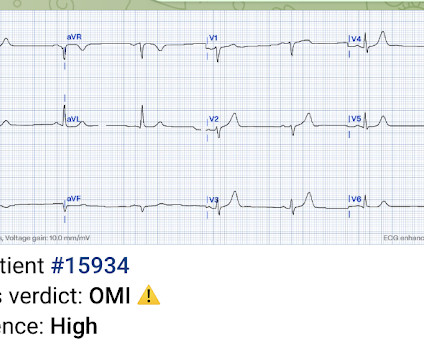
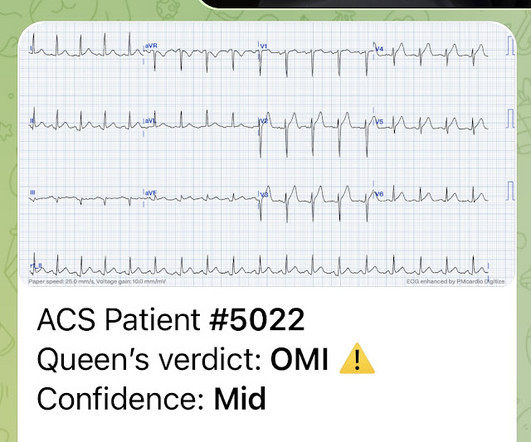
It is from a 50-something with chestpain: What do you think? This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria.
There was apparently no syncope and he had no bony injuries, but he did complain of left sided chestpain. His chest was tender. Is there STEMI? A bedside cardiac ultrasound was normal. An ECG was recorded: Avinash was understandably confused by this ECG. He wrote: "ECG 1 - shows wide ???IVCD IVCD type rhythm ??
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chestpain that started on the morning of presentation at around 8am. So it is very unclear to me whether or not "posterior STEMI" is actually a recognized entity under our current guidelines.
Algorithm: Veritas (on Mortara machines) The Queen gets it right Case 2 A middle-aged woman with chestpain and a "normal" ECG in triage. Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? Pain was resolving. The OMI was not seen and she arrested in triage.
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. Here is the clinical story: A 40 year old male with no cardiac history presented with acute substernal chestpain that started 40 minutes prior to arrival. This ECG was texted to me with no other information. What did I say?
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He was given aspirin and sublingual nitro and the pain resolved. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. He was started on nitro gtt.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
He was a 30-something with chestpain. Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. A male in his 30's complained of sudden severe substernal chestpain. Interventionalist at the Receiving Hospital: "No STEMI, no cath.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Jernberg T, et al.
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion. Learning Points: 1.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The day prior to presentation (about 12 hours prior to presentation) he described sudden onset chestpain and shortness of breath while gardening in his back yard. He had no further pain and went to bed that night with no complaints.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." The following ECG was obtained.
Sent by anonymous, edited by Pendell Meyers A man in his 50s with history only of hypertension presented with acute chestpain that started 45 minutes prior to presentation while doing yard work. Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10."
A 40-something woman presented to the ED having had “heartburn” overnight and then worsening chestpain 1 hour prior to arrival. T his is a systematic failure that has been documented in the following study: Garg A, Lehmann MH. OMI often does not meet STEMI criteria. The patient looked ill. Circ Arrhythm Electrophysiol.
The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. To me, that is a meaningless diagnosis. Here is the main learning point: The infarct was due to an occluded artery (Occlusion MI, OMI). In 30% of OMI, there is no significant ST Elevation.
A 50-something man with history only of alcohol abuse and hypertension (not on meds) presented with sudden left chestpain, sharp, radiating down left arm, cramping, that waxes and wanes but never goes completely away. persistent pain despite medical Rx brought emergently to Cath lab." It was not a STEMI) 1.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
A 40-something woman had sudden chestpain. This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI.
The combination of absence of chestpain and history of LV aneurysm made it easy to assess that this patient does not have acute OMI. At this point — I learned a bit more about today's patient: The patient is a man who had an inferior STEMI in 2010. We know today's patient had a documented inferior STEMI in 2010.
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". See this case: Pericarditis, or Anterior STEMI?
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. His vitals were normal and his first ECG was as shown below: There is obvious ST segment elevation (STE) in anterior leads.
This is why it is essential that the OMI/NOMI paradigm replace the STEMI/NonSTEMI paradigm. Under Non-STEMI, this patient would not have intervention until at least 20 hours (next day), after the infarct is completed. Learning Points: 1. 25-30% of OMI are not treated in a timely way.
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. This is a high troponin (most STEMI are above 10 ng/mL for troponin I). There is no STE or STD in III an aVF. Lead aVR has a bit of STD (reciprocal, as changes in lead aVR always are). There are also new very tiny Q waves in V4-6.
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. Learning Points: Currently by definition, there is unfortunately no such thing as a formal diagnosis of STEMI or STEMI criteria in the setting of RBBB and LAFB.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. He had no previously documented medical problems except polysubstance use. The patient continued having chestpain.
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. HR 40, BP 135/70, RR16, O2 100%.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. The physician documented “normal sinus rhythm”.
Triage documented a complaint of left shoulder pain. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
A late middle-aged man presented with one hour of chestpain. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." If the patient is at 1.8,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content