This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
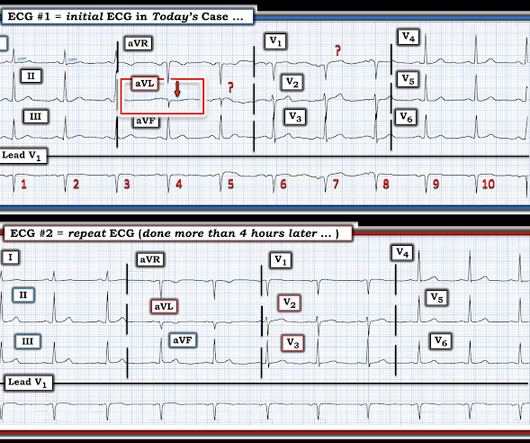
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
A 40 something woman with a history of hyperlipidemia and additional riskfactors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". The source of this case is anonymous.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Pain largely resolved prior to EMS arrival but completely subsided after prehospital NTG and aspirin. Triage EKG: What do you think?
Understanding Cardiovascular Disease in Women Understanding cardiovascular disease in women involves recognizing unique riskfactors such as hormonal changes and pregnancy-related complications, necessitating proactive care and awareness to manage and prevent heart disease effectively.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
The connection between heart health, vascular riskfactors, and sexual function is well-documented, with poor cardiovascular health often leading to or exacerbating erectile issues. The aim is to restore proper blood flow to the heart, alleviating symptoms like chestpain (angina) and reducing the risk of heart attacks.
A late middle-aged man presented with one hour of chestpain. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III. He had recently had a NonSTEMI.
3,4 Importantly, women have numerous sex-specific riskfactors in addition to non-sex-specific ones. Oral contraceptives and hormone replacement therapy can also affect risk, based on a woman's level of cardiometabolic risk. This is one way that multidisciplinary care comes into play.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. Bayes de Luna, A et al. Is this Type 2 Brugada syndrome/ECG pattern?
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. Three years later, the patient presented again to the ED with chestpain. Also : See Ken Grauer's excellent comments at the bottom.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." Unexplained cardiac arrest or documented VF/polymorphic VT: +3 3. The temperature was 39.5 Clinical History 2.a.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content