This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
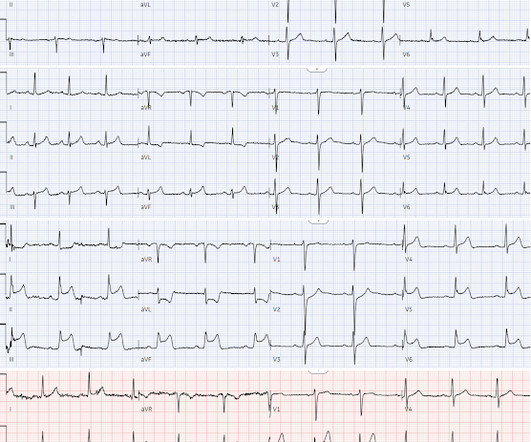
Written by Jesse McLaren A 45-year-old presented with 24 hours of intermittent chestpain. On it’s own this is nonspecific, but in the right context this could be diagonal occlusion (if active chestpain) or infero-posterior reperfusion (if resolved chestpain). #2 Can you guess the sequence?
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
The primary endpoint was the incidence of device syndrome, a composite of patient-reported symptoms (chestpain, palpitations, migraines, dyspnea, and rash).Results:Of No significant differences were observed in documented arrhythmias, bleeding, or stroke. Nickel hypersensitivity was assessed using skin patch testing.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think?
Written by Jesse McLaren Four patients presented with chestpain. The above said — the unfortunate reality ( as documented in Dr. McLaren's excellent discussion ) — is that subtle OMIs that can ( and should ! )
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc. This was written by Sam Ghali ( @ EM_RESUS ), with a few edits by me.
Submitted by Dr. Dennis Cho (@DennisCho), written by Jesse McLaren A 70-year-old with no cardiac history presented with 2 hours of chestpain radiating to the neck, associated with shortness of breath. As he documented, “This patient is experiencing chestpain consistent with an acute coronary syndrome.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chestpain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Anxiety is a common cause of chestpain with tachycardia.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). The patient was still with ongoing chestpain at the time ECG #1 was done.
There was apparently no syncope and he had no bony injuries, but he did complain of left sided chestpain. His chest was tender. A bedside cardiac ultrasound was normal. An ECG was recorded: Avinash was understandably confused by this ECG. He wrote: "ECG 1 - shows wide ???IVCD IVCD type rhythm ??
These were texted to me only with "chestpain." It helps to know that the patient has active chestpain, as Wellen's is a post occlusion (reperfusion) state, with open artery and pain-free. Smith and Meyers containing thousands of tracings with documentation of cardiac catheterization results. It was indeed.
It is from a 50-something with chestpain: What do you think? Up until recently — all computerized ECG interpretation programs that I am aware of used standard millimeter-based STEMI critieria as the basis for determining which chestpain patients should "qualify" for prompt cath with PCI. This was sent to me by a friend.
. = I had a previous case of an adolescent with trauma and chestpain who also had AIVR: An adolescent with trauma, chestpain, and a wide complex rhythm From this blog post: "AIVR is NOT common in otherwise healthy children.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
Case 2: A 57-year-old female was admitted to the hospital due to recurrent chestpain after physical activity for more than four years. Additionally, septum decreased from 16 to 13 mm after ten months, and the morphological changes associated with SVS also disappeared.
We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
Advanced cardiac imaging especially in atypical presentations, can aid in early diagnosis.Case:A 59 year-old man with history of biopsy-proven pulmonary sarcoidosis presented with non exertional chestpain for 2 months. EKG, cardiac enzymes, and Initial echocardiogram(TTE) was unremarkable.
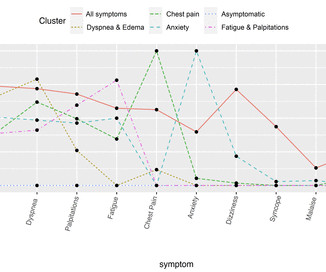
The most frequently documented symptoms were dyspnoea (64%), oedema (62%) and palpitations (57%). We identified six symptom clusters: generally symptomatic, dyspnoea and oedema, chestpain, anxiety, fatigue and palpitations, and asymptomatic (reference). female, 58% white).
Algorithm: Veritas (on Mortara machines) The Queen gets it right Case 2 A middle-aged woman with chestpain and a "normal" ECG in triage. Algorithm is either Glasgow or Marquette 12 SL The Queen gets it right Case 7 Chestpain relieved by Maalox and viscous lidocaine. The OMI was not seen and she arrested in triage.
(In other words, the artery was occluded but has sponteneously reperfused, resulting in pain relief) It is important to monitor patients with Wellens' syndrome for re-occlusion, which is usually, but not always, associated with recurrent chestpain. The patient remained pain free. ChestPain scores can be misleading.
Manifestations of CVDs, such as chestpain, abnormal serum markers, unstable angina, myocardial infarction (MI), myocarditis, and new-onset hypertension, were documented. The most common symptom was left hemithorax and interscapular pain (317 patients, 46%).
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
Here is the clinical story: A 40 year old male with no cardiac history presented with acute substernal chestpain that started 40 minutes prior to arrival. In spite of a relatively short QTc of 376 ms, the very low R-wave amplitude in V4 and the ST Elevation at 60 ms after the J-point in lead V3 contribute to a high final value.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." The following ECG was obtained.
He was a 30-something with chestpain. A male in his 30's complained of sudden severe substernal chestpain. This is the longest lasting I have ever documented a hyperacute T wave without going "up" or "down." Shoulder pain after lifting a heavy box de Winter's -- they remained stable for 30 minutes with many ECGs.
The providers documented concern for ST elevation in the precordial and lateral leads as well as a concern for hyperkalemic T waves in the setting of succinylcholine administration. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!) Potassium resulted as 4.9,
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Jernberg T, et al.
A 40-something woman presented to the ED having had “heartburn” overnight and then worsening chestpain 1 hour prior to arrival. T his is a systematic failure that has been documented in the following study: Garg A, Lehmann MH. In a patient with new-onset chestpain — this is diagnostic of acute OMI until you prove otherwise.
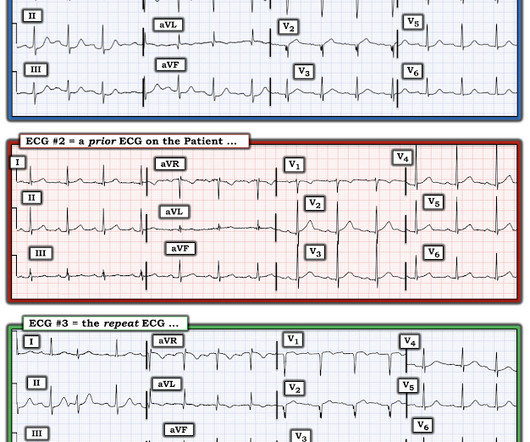
The reason the initial ECG is so concerning — is that it already suggests high likelihood of OMI ( = O cclusion-based MI ) in this 50-ish year old man who presents with a 2-hour history of new chestpain. What Do We Learn from ECG #3 ? Q waves are now present in each of the inferior leads in ECG #3.
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. He presents with an episode of brief, new-onset chestpain that had resolved by the time E CG # 1 was obtained.
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". The source of this case is anonymous.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. His vitals were normal and his first ECG was as shown below: There is obvious ST segment elevation (STE) in anterior leads.
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach. ST depression that is maximal in leads V2-to-V4.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The day prior to presentation (about 12 hours prior to presentation) he described sudden onset chestpain and shortness of breath while gardening in his back yard. He had no further pain and went to bed that night with no complaints.
The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain. 2-3 days after this he developed the same sharp chestpain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG.
And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now? Finally — Note that the S1Q3T3 pattern is missing in ECG #2 , despite documentation of a massive PE.
The combination of absence of chestpain and history of LV aneurysm made it easy to assess that this patient does not have acute OMI. In view of the History with the current admission ( ie, presenting to the ED for vertigo — with no new chestpain ) — I interpreted ECG #1 as no OMI.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chestpain that started on the morning of presentation at around 8am. Here is his triage ECG when he presented at 1657: What do you think?
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. In this patient with documented coronary disease — these q waves could reflect prior lateral infarction ( especially in view of the Q in lead aVL ). Time zero What do you think? There is inferior ST elevation. Pericarditis?
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The operator documented thoughtful consideration of risks and benefits of stent placement. Unfortunately, a few hours later the patient complained of recurrent chestpain. She took an oxycodone and called EMS.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content