This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
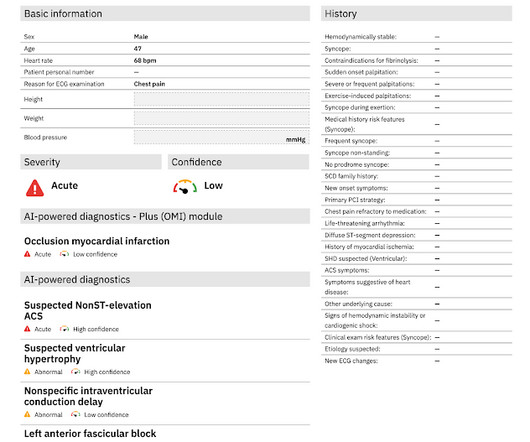
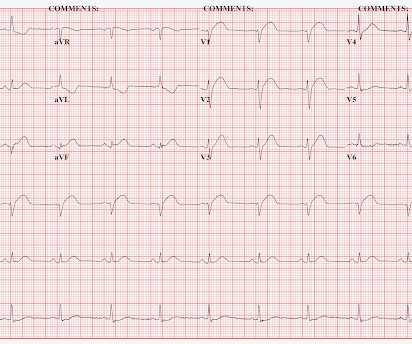
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
A 55 years old diabetic male patient who had 12 stents in his heart underwent a successful beating heart bypass surgery under Dr. Prateek Bhatnagar, Director Cardiac Surgery. The patient was suffering with angina (chestpain) since 2002. The last 3 stents were placed just 6 months back but were not working.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. The pain did not resolve with NTG, and so he went to emergent angiography: 1. LAD: severe in-stent restenosis in the mid (80%) and distal (90%) segment and diffuse disease distally.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. Without them the diagnosis is often tough and one must often rely on other clinical data- serial ECG’s, troponin, on-going chestpain, etc. She received PCI with 2 drug-eluting stents in overlying fashion.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. <0.049 ng/mL).
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. He also stated his arms and head feel "heavy" and he had a headache, dry heaves, and dizziness, and some "indigestion" in his chest "like acid". An open 90% LAD was stented.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The patient said his chestpain was 4/10, down from 8/10 on presentation. RCA and PDA before and after, arrows indicating stented regions. The following ECG was obtained.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chestpain, nausea, vomiting and diffuse abdominal pain. It was stented. The patient was in DKA with an anion gap of 35, a glucose of 1128, and a K of 5.5
As age advances and depending on risk factors like heredity, smoking, high blood pressure and diabetes, fat build up occurs in these blood vessels. This can block smooth flow of blood and the person can develop chestpain. Coronary arteries are blood vessels supplying oxygenated blood to the heart.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. Fortunately, that is exactly what happened.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss.
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. He denied fevers and chills, abdominal pain, chestpain, or SOB. It was opened and stented. Patient stated his dry weight is around 85 kg. The emesis is non-bloody and non-bilious.
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. He has a history of known CAD, diabetes, and dyslipidemia. Both were stented. By pure clinical appearance, he looked like the textbook patient with acute MI.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. You must record frequent serial ECGs for patients with chestpain.
While men often report crushing chestpain as the most prominent symptom, women might experience subtler symptoms like shortness of breath, nausea, or back pain. Women might describe it as a tightness, pressure, or squeezing sensation rather than a sharp pain.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
However, recent studies have observed that people below 40 are also experiencing heart attacks due to high blood pressure, cholesterol, diabetes, smoking, obesity, a sedentary lifestyle, and social and mental stress. So, how do you recognize a heart attack? The sooner you identify the symptoms, the quicker you can take action.
All of the patients contacted EMS due to acute onset chestpain. The above ECG is from a 70 something male with chestpain. ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chestpain. Following the improvement in the ECG the patient's pain too improved drastically.
This was texted to me by a paramedic while I was out running one day: "54 yo male chestpain started at 1pm. History of diabetes type II and stent placement in 2018. I’m seeing hyperacute T waves III, aVF, down sloping depression I and aVL. What do you think? I responded: "Definite inferior OMI. And Right Ventricular.
Written by Willy Frick A man in his mid 30s with type 1 diabetes presented with two days of midsternal and epigastric pain, described as both "sharp" and squeezing." He said the pain was worse with supination and improved with upright posture. The patient was treated with aspirin and a GI cocktail, which did not help the pain.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He carries the diagnoses hyperlipidemia, hypertension, and diabetes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content