This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
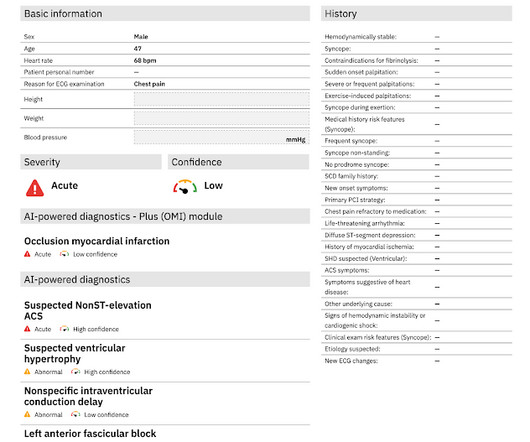
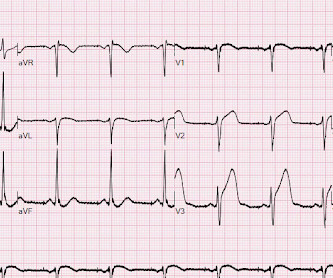
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. 2 years prior he had an angiogram which showed 90% proximal stenosis of the circumflex. The pain did not resolve with NTG, and so he went to emergent angiography: 1. LCX: non-dominant.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chestpain and diaphoresis, which recurred two hours prior to presentation. The chestpain was refractory to nitro so the cath lab was activated: 100% proximal LAD and 99% mid circumflex occlusions.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. 12:15 p.m.
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Here is his triage ECG: What do you think? The ECG was interpreted as non-ischemic.
We present a complex case of NSTEMI with multi-vessel coronary artery disease treated with PCI via the Carlino technique.Case Description:A 60-year-old female with a history of hypertension, diabetes mellitus, and ischemic heart disease presented with severe chestpain that radiated to the neck and was associated with nausea and vomiting.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The patient said his chestpain was 4/10, down from 8/10 on presentation. The LAD has diffuse disease with a few areas of moderate stenosis but no flow-limiting lesions.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Anything more on history?
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He went inside and sat down, and the pain slowly subsided over the course of about 30 minutes.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left.
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. He has a history of known CAD, diabetes, and dyslipidemia. There is evidence that de Winter's T-waves really represent a tiny trickle of blood through the thrombotic stenosis.
found that such ECG findings only represented left main ACS in 14% of such ECGs: Only 23% of patients with the aVR STE pattern had any LM disease (fewer if defined as 50% stenosis). Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? You probably think it is left main. No, hypokalemia.
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Vitals were within normal limits except for tachypnea.
A patient in their 40s with type 1 diabetes mellitus and hyperlipidemia presented to the emergency department with 5 days of “flu-like” illness. They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They denied fever, cough, dyspnea, and sick contacts.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
Most cases go undiagnosed until the condition advances enough to create symptoms such as shortness of breath, chestpain or fatigue. Valvular heart disease, a condition in which any of the heart’s four valves are damaged or diseased, afflicts 2.5 percent of all Americans and 13 percent of Americans over age 80.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. Below is a still image with the red arrow indicating the subtotal LMCA stenosis.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. The data is overwhelming every way you can possibly look at it. years of age versus 59.0±8.4
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He carries the diagnoses hyperlipidemia, hypertension, and diabetes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content