This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I came to work one day and one of my partners said, "Hey, Steve, we had a STEMI this afternoon!" Of course he said: "Yes, it was a 60 year old diabetic with Chestpain." That is not a STEMI. They had activated the cath lab and the interventionalist did not notice that it was not a STEMI/OMI. He said: "What?
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Past medical history included diabetes and hypertension.
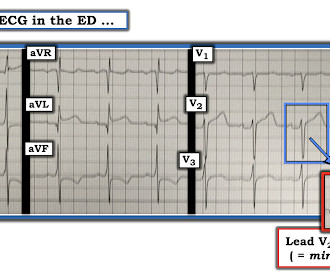
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). In STEMI, they are generally upright and large in proportion to the QRS. So this argues against acute STEMI.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chestpain and diaphoresis, which recurred two hours prior to presentation. It was signed off by an emergency physician as “STEMI negative” because it did not meet STEMI criteria.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. He also stated his arms and head feel "heavy" and he had a headache, dry heaves, and dizziness, and some "indigestion" in his chest "like acid". He had been awakened by cough at 3 AM 2 days earlier.
This ECG was texted to me with the message "A 31 year old with Diabetes and HTN complains of bilateral arm tingling and headache." The computer calls it a STEMI. If it was chestpain it would be more difficult to go with my gut on that." Never chestpain but had to treat as hypertensive emergency.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
Written by Pendell Meyers A woman in her 70s with diabetes, hypertension, and hyperlipidemia suddenly developed nausea, diaphoresis, and brief syncope while eating at a restaurant. She did not report any chestpain or pressure. This one likely does meet STEMI criteria in II, III, and aVF. Let me know what happens."
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Meets formal STEMI criteria in V2-V3.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He went inside and sat down, and the pain slowly subsided over the course of about 30 minutes.
Written by Pendell Meyers, sent by Anonymous A man in his 50s with history of type 2 diabetes, HTN, and HLD presented with one day of off and on chest / upper abdominal pain. It had awoken him from sleep earlier, and he described it as "gas pain," located in the upper epigastrium and radiating upwards.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chestpain, nausea, vomiting and diffuse abdominal pain. The possibility of anterior STEMI was not noticed during patient care. pH = 7.17, pCO2 = 24, HCO3 = 8.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. link] Harhash AA et al.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. There is some ST-segment elevation in DII, DIII, aVF, V4-6.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. OMI that are not STEMI can be very subtle and difficult to diagnose even though the findings are very specific.
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chestpain and shortness of breath off and on over the past three days, with associated vomiting. There is also much STE in V3-V6, especially V4-V6, that must be considered to be STEMI.
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. He denied fevers and chills, abdominal pain, chestpain, or SOB. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The patient said his chestpain was 4/10, down from 8/10 on presentation. The documentation does not describe any additional details of the history. ECG 1 What do you think?
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. He has a history of known CAD, diabetes, and dyslipidemia. Moreover, T-wave inversion in aVL was also found to be 100% sensitive and 86% specific for inferior STEMI. mm ST depression in aVL.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. He is an interventionalist in Turkey. A second ECG was taken at 15:16. Wait for the angiogram.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left.
Palpitations in a Young Healthy Male A pathognomonic ECG you should recognize instantly A middle-aged man with severe syncope, diffuse weakness Chestpain and Diffuse ST depression, with STE in aVR. Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? Are These Wellens' Waves??
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Vitals were within normal limits except for tachypnea.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Theiling BJ.
A 65 year old with diabetes presented with a syncopal episode while sitting, associated with weakness but no chestpain or shortness of breath. Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. You must record frequent serial ECGs for patients with chestpain.
All of the patients contacted EMS due to acute onset chestpain. The above ECG is from a 70 something male with chestpain. ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chestpain. All ECGs in this case have saddleback ST elevation. ECG #1 Case 1. ECG #3 Case 3.
Written by Willy Frick A man in his mid 30s with type 1 diabetes presented with two days of midsternal and epigastric pain, described as both "sharp" and squeezing." He said the pain was worse with supination and improved with upright posture. The patient was treated with aspirin and a GI cocktail, which did not help the pain.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). He presented to the emergency department for evaluation.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI".
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content