This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He had had several episodes of pain since onset; it was described as pressure-like and lasts about 5-15 minutes and resolves spontaneously. He had been pain free for about an hour. He had some "pre-diabetes ," but no h/o hypertension, no known family history of heart disease, and he smokes about 1-2 cigarettes per day.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chestpain. As per Dr. Smith — today's patient is a 40-something year old patient with severe diabetes, renal failure and known coronary disease — who presents with “acute crushing CP”.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. 40 mg of furosemide was given.
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. Ischemic Hyperacute T waves (Tall, round, symmetric, vs the “pointy” peaked-T’s of HyperK), are often a clue to ischemia. This was written by Sam Ghali ( @ EM_RESUS ), with a few edits by me. This case is tough.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chestpain and diaphoresis, which recurred two hours prior to presentation. The chestpain was refractory to nitro so the cath lab was activated: 100% proximal LAD and 99% mid circumflex occlusions.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. Take home 1.
Yang is also winner of the SCCT Best Abstract Award for his submission, “Coronary CT Angiography-derived Precursors Of Acute Coronary Syndrome In Ischemia-causing Lesions.” The SCCT Best Abstract Award is supported by the Cardiovascular Research Foundation of Southern California (CVRF of So.
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture. The most common “something else” symptom was shortness of breath.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. <0.049 ng/mL).
There is ST elevation in V1, and ST depression in V4-V6, suggestive of ischemia/MI. In this case the diagnosis was easy because the patient presented very ill with known Type I diabetes and with vomiting, not chestpain. What is the Diagnosis? --see due to DKA (pH 7.12, bicarb 6). There was no MI here. Thanks to K.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast.
This ECG was texted to me with the message "A 31 year old with Diabetes and HTN complains of bilateral arm tingling and headache." If it was chestpain it would be more difficult to go with my gut on that." Never chestpain but had to treat as hypertensive emergency. There is also STE in V2. What do you think?
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients. 12:15 p.m.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. The patient rapidly regained consciousness, reporting no residual pain.
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Here is his triage ECG: What do you think? The ECG was interpreted as non-ischemic.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. He also stated his arms and head feel "heavy" and he had a headache, dry heaves, and dizziness, and some "indigestion" in his chest "like acid". He had been awakened by cough at 3 AM 2 days earlier.
Written by Pendell Meyers A woman in her 70s with diabetes, hypertension, and hyperlipidemia suddenly developed nausea, diaphoresis, and brief syncope while eating at a restaurant. She did not report any chestpain or pressure. The morphology of STE is not diagnostic of being due to acute transmural ischemia.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Anything more on history?
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? non-occlusive ischemia) 2.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. He denied fevers and chills, abdominal pain, chestpain, or SOB. Normal RBBB, no evidence of ischemia. Patient stated his dry weight is around 85 kg. The emesis is non-bloody and non-bilious.
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. He has a history of known CAD, diabetes, and dyslipidemia. This post was written by one of our fantastic Hennepin County Medical Center Emergency Medicine interns who is an ECG whiz, Daniel Lee.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? ST depression: is it ischemia? J Electrocardiol 2013;46:240-8. Hypokalemia c.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He went inside and sat down, and the pain slowly subsided over the course of about 30 minutes.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. EKG shown here: LAFB with no clear signs of OMI or ischemia. Sent by Pete McKenna M.D. Triage ECG: What do you think?
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Monitor cholesterol levels and manage conditions like diabetes that can strain the heart. Cardiomyopathy Cardiomyopathy is a condition that affects the heart muscle, causing it to become enlarged, thick, or rigid.
Patients with coronary artery diseaseplaque buildup inside the arteries that leads to chestpain, shortness of breath, and heart attackoften undergo PCI, a non-surgical procedure in which interventional cardiologists use a catheter to place stents in the blocked coronary arteries to restore blood flow.
In MSIMI (Mental Stress-induced Myocardial Ischemia) studies , mental stress activities like public speaking were evaluated for their impact on ischemia, measured via myocardial SPECT and vascular function (microvascular function, endothelial function). Therapy with her pastor was preferred.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
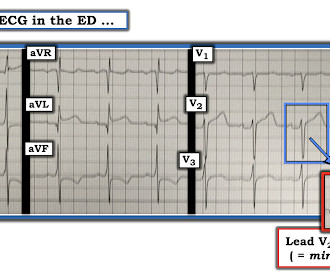
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Lead V2 shows RR’ QRS configuration, and although ST depression is otherwise expected here, the discordance is a bit excessive.
All of the patients contacted EMS due to acute onset chestpain. The above ECG is from a 70 something male with chestpain. ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chestpain. All ECGs in this case have saddleback ST elevation. ECG #1 Case 1. ECG #3 Case 3.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. He presented to the emergency department for evaluation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content